|
|
Post by stevil on May 9, 2019 0:14:51 GMT -5
Notice he did vote for its approval though! And I highly doubt he was being serious... Probably was saying it tongue in cheek. Endos do a ton more than just diabetes. They also handle the pituitary, hypothalamus, pineal gland, adrenals, reproductive organs, etc. There will always be a need for an endocrine. Would they notice a hit to their business if diabetes becomes well-managed? Absolutely. However, they'll still be managing diabetes. Not every referral is because a doctor doesn't know how to manage therapy. There is still a lot of business to share because PCP's don't want to deal with stuff. One of many reasons PCPs chose not to specialize is because they don't want to get sucked into seeing only one patient population. Someone still has to write the scripts for diabetics. Endos will be fine. I'm a non-diabetic endo patient and couldn't manage to get one for regular care under my health plan because they are all too busy and not accepting new patients. I'd look forward to some freeing up. Agree, they will do well, as all specialists tend to even with less people with uncontrolled diabetes. Sadly, there is an over abundance of patients with diabetes. Special thanks to those docs that go into primary care. Look forward to hearing where you end up Stevil. Crazy enough, if the "self-reported" income charts are to be believed, endos are actually near dead last only to peds docs on the pay scale. Reimbursement sucks for endos, despite what one might be led to believe on here. I'm sure they'd love to have the same pay for much less complicated patients. I feel bad for those guys... Always sorting out messes and getting paid squat for it. |
|
|
|
Post by stevil on May 9, 2019 0:18:21 GMT -5
In other words, anyone who argues with Stevil is a "fool." Got it. Now it's really starting to feel like the old days. If that's how you chose to read my post, then I won't argue with you  |
|
|
|
Post by ktim on May 9, 2019 0:30:47 GMT -5
I'm a non-diabetic endo patient and couldn't manage to get one for regular care under my health plan because they are all too busy and not accepting new patients. I'd look forward to some freeing up. Agree, they will do well, as all specialists tend to even with less people with uncontrolled diabetes. Sadly, there is an over abundance of patients with diabetes. Special thanks to those docs that go into primary care. Look forward to hearing where you end up Stevil. Crazy enough, if the "self-reported" income charts are to be believed, endos are actually near dead last only to peds docs on the pay scale. Reimbursement sucks for endos, despite what one might be led to believe on here. I'm sure they'd love to have the same pay for much less complicated patients. I feel bad for those guys... Always sorting out messes and getting paid squat for it. Well, hopefully you have the heart to choose a specialty that is rewarding or the brains to choose one that is financially rewarding. Hopefully we have the intelligence to stop creating such a dichotomy in medicine, with such high costs for education and disparate pay. "Sorting out messes"... isn't that what you're signing up for? |
|
|
|
Post by stevil on May 9, 2019 0:49:25 GMT -5
Yes and no. Right now, the current guidelines call for statins and Ace inhibitors/ARBs for all patients on insulin. So any insulin dependent diabetic is a baked in level 4 billing code (out of 5). So whether the patient is well-controlled or not... Depending on how badly controlled they are, they may qualify for a level 5 code, but it's much harder to justify level 5s than 4s...
In other words, it's not uncommon to get paid the same for a super complicated patient as one who is well-controlled. But you do far more work for the one that's not controlled and carry more risk as a physician for the same pay.
|
|
|
|
Post by sayhey24 on May 9, 2019 5:26:36 GMT -5
Stevil - most of the business Endo's do is out of control T2s. You get a good T2 and they are a gold mine. The out of control sugars have destroyed all kinds of things from the eyes to the toes. I can tell you with 100% certainty the Endo at the ADCOMwas completely serious and he was right. As you approach 40 and your thought process matures what you will realize is there are only about 15 years left to make the money to live the dream. For the Endo every PWD is a pay day. Once PCPs start prescribing afrezza day 1 instead of metformin and have their patients sign up for a connected care service the big Endo pay day is gone.They will go the way of the flip phone, they are still around. That is flat out wrong. Endos make no money from complications. That is all handled by other specialists; surgeons, dialysis clinics, ophthalmologists, and cardiologists. So an out of control T2 is definitely not a gold mine for the endo. The last paragraph is the most ill-informed. Typically a PCP will deal with any non-insulin using Type 2, early treatment of Type 2 is a PCP and not Endo decision. Endo's usually only get involved after metformin and a follow on has failed. The purpose of an SoC is to distill the body of knowledge so a PCP can follow the flow chart to treat the patient knowing he is following the the current best practice. Aged - I am not sure what you are talking about. The first complication is high blood sugar. The last I checked Endos are treating this. Then its hypoglycemia because the insulin they give them is as Al Mann said "too damn slow". This is one pay day after the next. Without the hypos, bringing down the high sugar would be easy. The early decision of how to treat T2s is clearly being controlled by the Endos. Who do you think is controlling the SOCs? Its not the PCPs. The PCP are just following what the ADA is telling them to do. Give them metformin is what the SOC says the last I checked. There is no need for the SOC chart now that we have afrezza. Give them the afrezza and you don't need all the "Steps". Then again a huge part of the Endo business goes away too. The current SOC is a "Treat to Fail" protocol and as the "Father" of metformin approval in the U.S. - Dr. Ralph DeFronzo now says after he has learned the hard way “The most waste in type 2 diabetes is to continuously put people on metformin and sulfonylureas (glyburide, glimepiride, etc.). These drugs have no protective effect on the beta cell, and by the time you figure out what you’re doing, there are no beta cells left to save.” – Dr. Ralph DeFronzo (University of Texas Health Science Center) diatribe.org/the-diatribe-foundation-and-tcoyd-11th-annual-forum |
|
|
|
Post by uvula on May 9, 2019 7:53:33 GMT -5
Mnkd to hold 2019 first quarter financial results on may 7.
|
|
|
|
Post by ktim on May 9, 2019 8:06:24 GMT -5
Medicare and Medicaid would not cover clinics that are owned by a pharma to push their own products. I doubt commercial health insurance would either. Does Medicare and Medicaid pay for Cigarettes? The average pack is over $6 per day more than the daily cost of afrezza insulinsavings.com Now commercial health insurance pays for health and wellness clinics such as Weight Watchers www.weightwatchers.ca/util/art/index_art.aspx?tabnum=1&art_id=134541&sc=3046Its not a question of can Mannkind partner with someone to do this, yes they can. Its a question of structuring the deal properly and doing it. It can not be "Diabetes" clinic. They need to be health and wellness centers dealing in weight loss and fitness. There is a huge untapped market in the weightloss business for CGM technology and connected care and guess what - about 25% of these people are PWDs and many don't even know it. Not on Medicare yet, but no, I'm pretty sure they don't pay for cigarettes. Not sure what that has to do with what I posted. They can both not pay for cigarettes and not pay for pharma owned clinics. You'd have to explain the relevance of that comment if there is any. As for commercial insurance, the first step would be making Afrezza preferred on their formulary before they start adding MNKD owned clinics to their provider networks. Theoretically "partnering" at a commercial level with anyone to do anything is possible. It's just a question of whether there are two parties for which it makes economic sense within the prevailing business dynamics of an industry. Perhaps you know things that MNKD management does not, or perhaps the other way around. You can always contact them and tell them about your clinic idea. I suspect others have. If you think they are simply negligent in not doing it, you can get on board with the change management crowd. |
|
|
|
Post by ktim on May 9, 2019 8:14:02 GMT -5
Yes and no. Right now, the current guidelines call for statins and Ace inhibitors/ARBs for all patients on insulin. So any insulin dependent diabetic is a baked in level 4 billing code (out of 5). So whether the patient is well-controlled or not... Depending on how badly controlled they are, they may qualify for a level 5 code, but it's much harder to justify level 5s than 4s... In other words, it's not uncommon to get paid the same for a super complicated patient as one who is well-controlled. But you do far more work for the one that's not controlled and carry more risk as a physician for the same pay. What does the billing code level mean? Does that mean a doctor can charge more for a standard office visit if a patient is at a higher "level" regardless of what is actually done during the visit? |
|
|
|
Post by agedhippie on May 9, 2019 9:02:45 GMT -5
That is flat out wrong. Endos make no money from complications. That is all handled by other specialists; surgeons, dialysis clinics, ophthalmologists, and cardiologists. So an out of control T2 is definitely not a gold mine for the endo. The last paragraph is the most ill-informed. Typically a PCP will deal with any non-insulin using Type 2, early treatment of Type 2 is a PCP and not Endo decision. Endo's usually only get involved after metformin and a follow on has failed. The purpose of an SoC is to distill the body of knowledge so a PCP can follow the flow chart to treat the patient knowing he is following the the current best practice. Aged - I am not sure what you are talking about. The first complication is high blood sugar. The last I checked Endos are treating this. Then its hypoglycemia because the insulin they give them is as Al Mann said "too damn slow". This is one pay day after the next. Without the hypos, bringing down the high sugar would be easy. The early decision of how to treat T2s is clearly being controlled by the Endos. Who do you think is controlling the SOCs? Its not the PCPs. The PCP are just following what the ADA is telling them to do. Give them metformin is what the SOC says the last I checked. There is no need for the SOC chart now that we have afrezza. Give them the afrezza and you don't need all the "Steps". Then again a huge part of the Endo business goes away too. The current SOC is a "Treat to Fail" protocol and as the "Father" of metformin approval in the U.S. - Dr. Ralph DeFronzo now says after he has learned the hard way “The most waste in type 2 diabetes is to continuously put people on metformin and sulfonylureas (glyburide, glimepiride, etc.). These drugs have no protective effect on the beta cell, and by the time you figure out what you’re doing, there are no beta cells left to save.” – Dr. Ralph DeFronzo (University of Texas Health Science Center) diatribe.org/the-diatribe-foundation-and-tcoyd-11th-annual-forumIn the first, and most, cases bringing hyperglycemia under control is handled by PCPs for T2. In diabetes endos are almost entirely focused on T1 and insulin using T2. Hyperglycemia is not thought of as a diabetic complication, but diabetic complications are often caused by hyperglycemia. Some are caused by other aspects of diabetes. There are a lot of treatments to bring down high levels, DeFronzo's favorite is SGLT-2 for example. One which is receiving a lot of attention at the moment is combining basal insulin and GLP-1. You are perfectly correct about DeFronzo's opinion of metformin and he now ranks it as his 4th choice for a starting treatment with SGLT-2 as the favorite, and GLP-1 in second place. Insulin is not on his list. The SoC is a way to scale the treatment of diabetics, especially T2. It's driven by endos who base their decisions on a clear methodology with large scale trial data as the most influential. If there is no solid trial data to support a change it isn't going to happen. If you want to see the direction treatment is going look at the ADA - EASD joint statement as this drives future direction. |
|
|
|
Post by mnkdfann on May 9, 2019 9:09:36 GMT -5
The current SOC is a "Treat to Fail" protocol and as the "Father" of metformin approval in the U.S. - Dr. Ralph DeFronzo now says after he has learned the hard way “The most waste in type 2 diabetes is to continuously put people on metformin and sulfonylureas (glyburide, glimepiride, etc.). These drugs have no protective effect on the beta cell, and by the time you figure out what you’re doing, there are no beta cells left to save.” – Dr. Ralph DeFronzo (University of Texas Health Science Center) The SoC is a way to scale the treatment of diabetics, especially T2. It's driven by endos who base their decisions on a clear methodology with large scale trial data as the most influential. If there is no solid trial data to support a change it isn't going to happen. If you want to see the direction treatment is going look at the ADA - EASD joint statement as this drives future direction. Thank goodness Kendall said his task of changing the SOC to favour Afrezza is the easiest job he's ever had (or similar words to that effect). |
|
|
|
Post by liane on May 9, 2019 9:19:45 GMT -5
Yes and no. Right now, the current guidelines call for statins and Ace inhibitors/ARBs for all patients on insulin. So any insulin dependent diabetic is a baked in level 4 billing code (out of 5). So whether the patient is well-controlled or not... Depending on how badly controlled they are, they may qualify for a level 5 code, but it's much harder to justify level 5s than 4s... In other words, it's not uncommon to get paid the same for a super complicated patient as one who is well-controlled. But you do far more work for the one that's not controlled and carry more risk as a physician for the same pay. What does the billing code level mean? Does that mean a doctor can charge more for a standard office visit if a patient is at a higher "level" regardless of what is actually done during the visit? Yes. The way the crazy system runs right now, the more chronic conditions you are managing, or if a condition is worsening, the more "Medical Decision Making" and this can bump up the level of a visit. It has been proposed for Jan 2021 to essentially combine levels 2 - 4 under the same level of pay. And it would require far less documentation (which is the bane of our existence right now). Level 1 is essentially a nurse visit. And level 5 is indeed very complex and difficult to meet, and will raise audit eyebrows. |
|
|
|
Post by peppy on May 9, 2019 9:58:39 GMT -5
Yes and no. Right now, the current guidelines call for statins and Ace inhibitors/ARBs for all patients on insulin. So any insulin dependent diabetic is a baked in level 4 billing code (out of 5). So whether the patient is well-controlled or not... Depending on how badly controlled they are, they may qualify for a level 5 code, but it's much harder to justify level 5s than 4s... In other words, it's not uncommon to get paid the same for a super complicated patient as one who is well-controlled. But you do far more work for the one that's not controlled and carry more risk as a physician for the same pay. I did not know that. How is medicine handling that secondary to statins (with out the cholesterol) the co enzyme Q10 can not be made and the effect that has on the electron transport in cellular respiration? ![]() 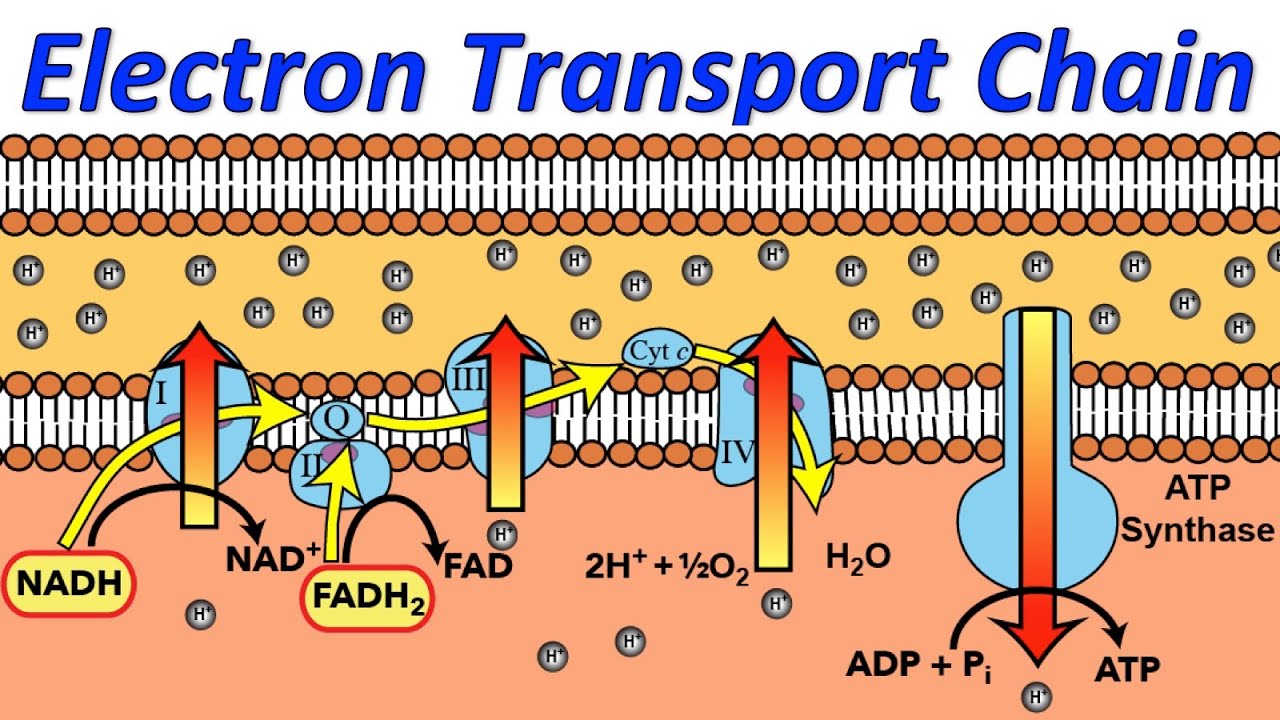 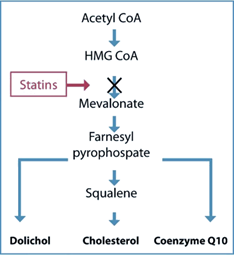 ![]() |
|
|
|
Post by mango on May 9, 2019 11:05:30 GMT -5
Yes and no. Right now, the current guidelines call for statins and Ace inhibitors/ARBs for all patients on insulin. So any insulin dependent diabetic is a baked in level 4 billing code (out of 5). So whether the patient is well-controlled or not... Depending on how badly controlled they are, they may qualify for a level 5 code, but it's much harder to justify level 5s than 4s... In other words, it's not uncommon to get paid the same for a super complicated patient as one who is well-controlled. But you do far more work for the one that's not controlled and carry more risk as a physician for the same pay. I did not know that. How is medicine handling that secondary to statins (with out the cholesterol) the co enzyme Q10 can not be made and the effect that has on the electron transport in cellular respiration? ![]() ![]()  |
|
|
|
Post by peppy on May 9, 2019 11:11:51 GMT -5
I had no clue, the electron transport system/chain is how the energy is created to make the ATP.
The electrons provide the energy to make it tri.
Statins effect the electron transport chain, in every cell.
Additionally something else I was not aware of until recently, is while each cell has mitochondria, cells have multiple mitochondria.
Charge has made medicine more interesting.
|
|
|
|
Post by mango on May 9, 2019 12:16:49 GMT -5
I did not know that. How is medicine handling that secondary to statins (with out the cholesterol) the co enzyme Q10 can not be made and the effect that has on the electron transport in cellular respiration? ![]() ![]() The electron transport system is pretty cool |
|











