|
|
Post by peppy on Oct 27, 2022 15:46:51 GMT -5
The perspective that it's a mistake to believe Afrezza will help or fix the problem implies that something else exists that will. What would that be? Or is it the belief that all options are treat-to-failure? Just wondering. To be clear here; the problem that is being fixed is Type 2 diabetes. Will Afrezza help? Absolutely - it's a fast insulin with rapid clearance and reliable absorption. Will it fix Type 2? Depends what fix means - taken to be fix systemic insulin resistance, there is no evidence to support this and it seems unlikely to me since the problem is on the utilization rather than availability side.All options except insulin are treat to fail. Insulin isn't TTF because you can always add more insulin so it cannot fail. However,, historically you will need to progressively increase your insulin dosage as diabetes progresses, and you get the issues Stevil talked about from excessive insulin. If it is claimed there is no long term progression with Afrezza then that needs to be evidenced with trials (treat to target) and not just claimed. quote, systemic insulin resistance, the problem is on the utilization rather than availability side. reply, amazing medicine doesn't have a clue as to what causes this resistance and utilization problem? What could it be? ![]() 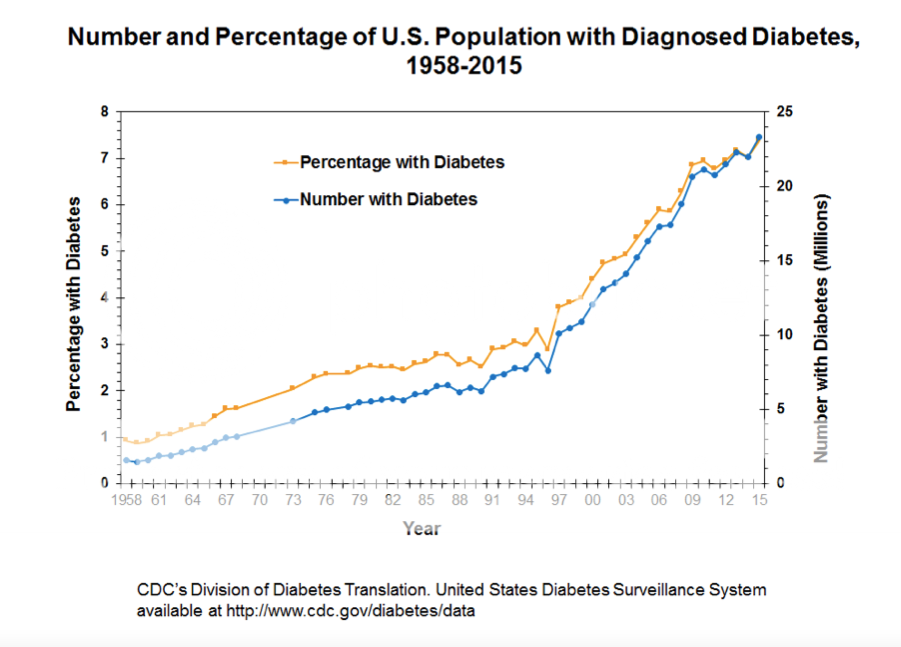 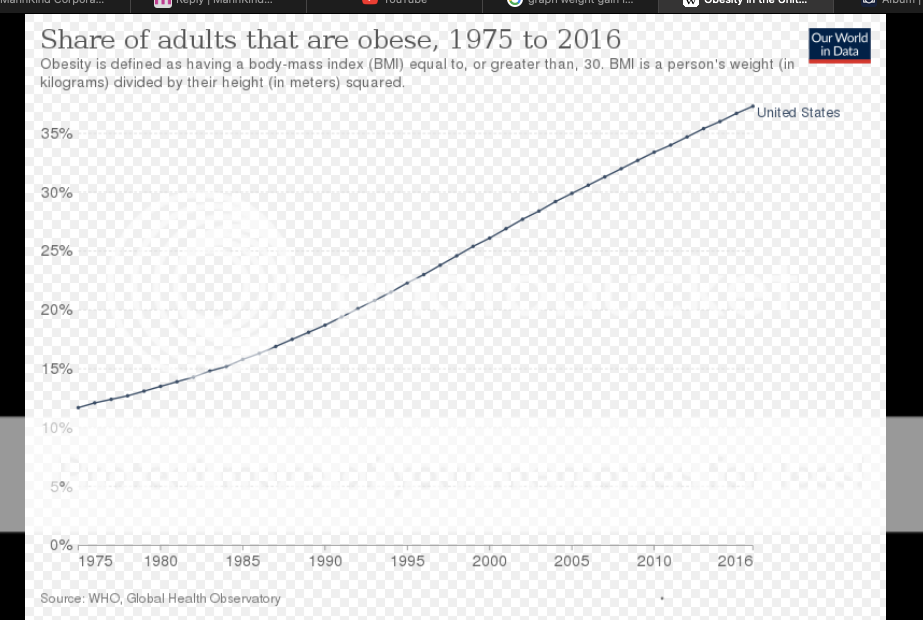 |
|
|
|
Post by runner on Oct 27, 2022 20:50:16 GMT -5
Wow, from 1% of the population to 7% of the population in 57 years. Plus, the population itself grew by about 40% over that period of time. I feel so fortunate that none of my immediate family has been affected thus far.
Interesting stats, Peppy. Thanks
|
|
bkdmd
Researcher

Posts: 79
|
Post by bkdmd on Oct 28, 2022 11:13:15 GMT -5
Since Mohammad Ali won his first heavy weight title, the average weight of both men and women in the USA is up about 30 pounds.
I have a friend who works in fashion. They intentionally make their clothes bigger two times a year. Once for hotter weather clothes and one time for winter weather clothes because people will not buy as many new clothes if they have to buy a bigger size.
|
|
|
|
Post by sayhey24 on Oct 28, 2022 12:32:58 GMT -5
Peppy - to address the statement - "the problem is on the utilization rather than availability side". Its actually on both sides but on the utilization side its only on pancreatic released insulin. What we can demonstrate is if we give the afrezza before the BG spikes we need a lot less afrezza. I would think VDex is seeing the same. During this spiking process the pancreas has been pumping out what it has and it is continuing to try and pump out what it has to reduce the BG levels. Simply put - significant "insulin resistance" can be avoided by reducing phase 1/2 pancreatic release. In other words - afrezza gets utilized pretty darn good the more we can reduce pancreatic release. On the availability side what we know and have known for a very long time since they started autopsying pancreases 100 years ago is beta cell mass will increase in the non-diabetic obese. They also fattened up the pigs before pancreas extraction for insulin. There are many studies on the subject but this one I find interesting because it was done during Covid - www.ncbi.nlm.nih.gov/pmc/articles/PMC7766247/The simple question is - why are most fat people not diabetic? If being fat made you diabetic then most fat people should be but they are not. The nondiabetic obese will grow more beta cells and produce more insulin and it gets utilized just fine. The healthy body (even if obese) will adapt to the body's need for insulin. In the diabetic who can be fat or thin they lose beta cell mass. As an aside, when my dad was first diagnosed as a T2 he was pretty fit but his eyesight started to go and driving at night with lights is what made him go to the doctor. As time went on he started putting on the weight even though he did not snack nor drink and he nearly cut out all sugar products like cakes, candy and soda. He was convinced that having a Coke at lunch was why he developed T2. His weight gain is similar to what the tech diet companies are seeing. They are seeing post prandial loss prior to weight gain. |
|
|
|
Post by agedhippie on Oct 28, 2022 18:30:11 GMT -5
quote, systemic insulin resistance, the problem is on the utilization rather than availability side. reply, amazing medicine doesn't have a clue as to what causes this resistance and utilization problem? What could it be? There are lot of really technical explanations that I have always lost the will to follow before I reached the end, but fundamentally it seems to come down to genetics. The last time I looked at this which was a few years ago now they had identified 120 genes that they thought were involved in Type 2 diabetes. The problem is that this gives a huge number of possible combinations and only some of those combinations will cause diabetes. This is why a magic bullet is so unlikely - you have to hit literally hundreds of targets at once. Having decided that you are unlikely to cure Type 2 in the short term the second best option is to deal with the symptoms. This is why sort of why insulin has fallen from favor a bit, they want to modify the metabolism so you can live within your own insulin budget. I mentioned Actos earlier (not a drug I like) and it's a good example. Actos triggers receptors which cause your genes modify their behavior in a way that reduces insulin resistance. This gets you back into the normal range for a while (Type 2 is progressive although the rate of progression differs from person to person). To be clear here; insulin, Afrezza or otherwise does not reduce your systemic insulin resistance. What it will do is reduce your glucose related insulin resistance. If your levels are 300 it is going to take more insulin to get a 10 point drop than it will if your level is 150. This means, and why Afrezza works in this context, is if you can kill a spike early you need less extra insulin because the spike is smaller so the insulin resistance is less so you will get back to baseline faster - it's a virtuous circle. The systemic insulin resistance is unaltered by this behavior though and you are still going to require more total insulin (your own + external) than you should, just not as much as you might have  |
|
|
|
Post by peppy on Oct 28, 2022 19:19:03 GMT -5
quote, systemic insulin resistance, the problem is on the utilization rather than availability side. reply, amazing medicine doesn't have a clue as to what causes this resistance and utilization problem? What could it be? There are lot of really technical explanations that I have always lost the will to follow before I reached the end, but fundamentally it seems to come down to genetics. The last time I looked at this which was a few years ago now they had identified 120 genes that they thought were involved in Type 2 diabetes. The problem is that this gives a huge number of possible combinations and only some of those combinations will cause diabetes. This is why a magic bullet is so unlikely - you have to hit literally hundreds of targets at once. Having decided that you are unlikely to cure Type 2 in the short term the second best option is to deal with the symptoms. This is why sort of why insulin has fallen from favor a bit, they want to modify the metabolism so you can live within your own insulin budget. I mentioned Actos earlier (not a drug I like) and it's a good example. Actos triggers receptors which cause your genes modify their behavior in a way that reduces insulin resistance. This gets you back into the normal range for a while (Type 2 is progressive although the rate of progression differs from person to person). To be clear here; insulin, Afrezza or otherwise does not reduce your systemic insulin resistance. What it will do is reduce your glucose related insulin resistance. If your levels are 300 it is going to take more insulin to get a 10 point drop than it will if your level is 150. This means, and why Afrezza works in this context, is if you can kill a spike early you need less extra insulin because the spike is smaller so the insulin resistance is less so you will get back to baseline faster - it's a virtuous circle. The systemic insulin resistance is unaltered by this behavior though and you are still going to require more total insulin (your own + external) than you should, just not as much as you might have technical explanations come down to genetics. identified 120 genes that they thought were involved in Type 2 diabetes. If that is the case, explain this? Bariatric (Weight-Loss) Surgery for Treating Diabetes Weight-loss surgery, also called bariatric surgery, can be done in minimally invasive ways and can be used to treat Type 2 diabetes. The surgery treats diabetes by controlling how much sugar is in the blood. One type of surgery is called the duodenal switch. my.clevelandclinic.org/health/treatments/21153-bariatric-weight-loss-surgery-for-treating-diabetes Foods that are high in fats and carbohydrates increases fatty acids in the blood and lipid (fat) build-up in the liver and muscles. This increases insulin resistance and inflammation. Over time, the pancreas stops making enough insulin. 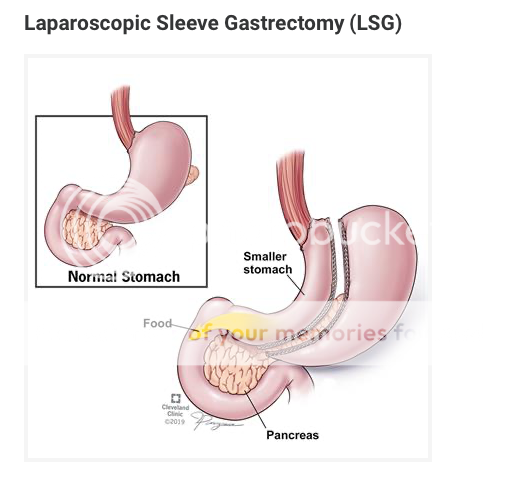 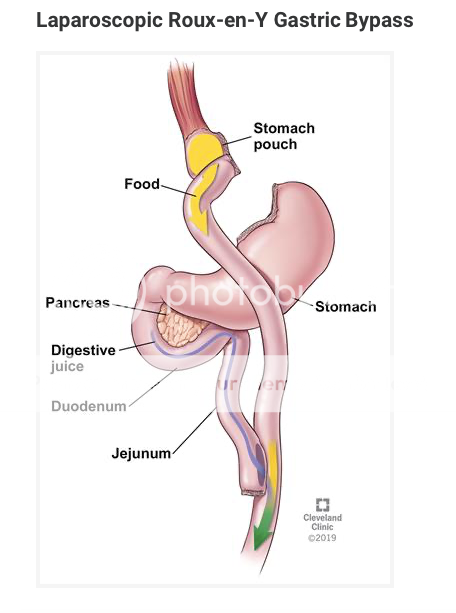 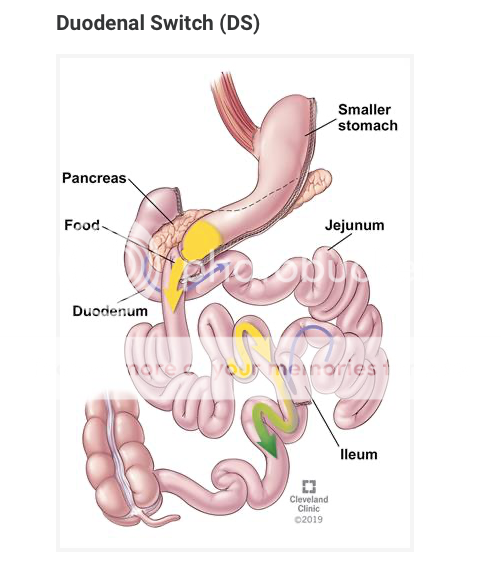 |
|
|
|
Post by sayhey24 on Oct 29, 2022 8:28:12 GMT -5
quote, systemic insulin resistance, the problem is on the utilization rather than availability side. reply, amazing medicine doesn't have a clue as to what causes this resistance and utilization problem? What could it be? There are lot of really technical explanations that I have always lost the will to follow before I reached the end, but fundamentally it seems to come down to genetics. The last time I looked at this which was a few years ago now they had identified 120 genes that they thought were involved in Type 2 diabetes. The problem is that this gives a huge number of possible combinations and only some of those combinations will cause diabetes. This is why a magic bullet is so unlikely - you have to hit literally hundreds of targets at once. Having decided that you are unlikely to cure Type 2 in the short term the second best option is to deal with the symptoms. This is why sort of why insulin has fallen from favor a bit, they want to modify the metabolism so you can live within your own insulin budget. I mentioned Actos earlier (not a drug I like) and it's a good example. Actos triggers receptors which cause your genes modify their behavior in a way that reduces insulin resistance. This gets you back into the normal range for a while (Type 2 is progressive although the rate of progression differs from person to person). To be clear here; insulin, Afrezza or otherwise does not reduce your systemic insulin resistance. What it will do is reduce your glucose related insulin resistance. If your levels are 300 it is going to take more insulin to get a 10 point drop than it will if your level is 150. This means, and why Afrezza works in this context, is if you can kill a spike early you need less extra insulin because the spike is smaller so the insulin resistance is less so you will get back to baseline faster - it's a virtuous circle. The systemic insulin resistance is unaltered by this behavior though and you are still going to require more total insulin (your own + external) than you should, just not as much as you might have Aged - if diabetes was genetic then identical twins would always develop diabetes together - they don't. This has been established for years. To address your statement "To be clear here; insulin, Afrezza or otherwise does not reduce your systemic insulin resistance" - think about what we can demonstrate. With the exact same carb load if we wait to take the afrezza the BG rises and stays high while the pancreas is releasing what it has. After it has spiked it takes 2x the afrezza to get it back down. If we take the afrezza before the pancreas has been working hard afrezza will bind to the receptors and get the BG back down for the same carb load. The same carb load should require the same amount of insulin give or take. This is why T1s do carb counting. This is pretty repeatable. You can try it yourself if you have a T2 friend with little post prandial control. Its not about the spike, its about the receptors using the insulin. The below paper thinks its the cytokines from the immune system. For sure we can see the beta cells virally infected. This is no longer up for debate as is beta cell mass loss not debatable. We can show both in the lab. As far as your comments on Actos I ignored it as TZDs have no place in T2 treatment as they have caused so much demonstrable harm. What does Actos do? It promotes fat cell growth which are new cells with new receptors. If we exercise we get new muscle cells with new receptors. Both are more insulin sensitive, why? Why are new receptors which have not been exposed to the pancreas's "insulin" more sensitive? If the Wensveens are correct about the cytokines we can take some guesses. ncbi.nlm.nih.gov/pmc/articles/PMC8050380/I do agree we are not going to "cure" T2. If the Wensveens are correct and if the Josil research from years ago was correct we have various viruses which attack the beta cells. Of course since covid we have a bunch of studies showing beta cell viral infection. What we can do is try to help the immune system do its job. The best way to do that is by taking the load off the pancreas and limit what its releasing. We have seen this in early insulin intervention studies. The good news is more and more studies are being done since covid looking at its connection to T2. The reality is as with covid there will be no cure. All we can do is promoted the immune system and provide some help for the pancreas by providing endogenous insulin which mimics pancreatic release. What we do need is a plan from Mike on how to leverage what we can demonstrate with afrezza and how we can crack into a market which is selling $40B a year in "treat to fail" snake oil. Al Mann did not put $1B of his own money into this on a whim. It would be nice to have Mike publicly say why he is taking afrezza as step 1 and not metformin or a GLP1. |
|
|
|
Post by agedhippie on Oct 29, 2022 9:21:20 GMT -5
Aged - if diabetes was genetic then identical twins would always develop diabetes together - they don't. This has been established for years. ... Not they don't develop diabetes together, and that is down to an epigenetic change over their lifetime. They start out identical, and as soon as they are born they start to develop independently due to environmental factors. Epigenetic change is one of the building blocks of genetics. If you are going on a gene hunt you are better off looking at places with homogenous gene pools which is why Finland and Iceland are extremely popular with medical researchers. For Type 2 diabetes it's the Pima Indians. |
|
|
|
Post by agedhippie on Oct 29, 2022 9:55:20 GMT -5
To address your statement "To be clear here; insulin, Afrezza or otherwise does not reduce your systemic insulin resistance" - think about what we can demonstrate. With the exact same carb load if we wait to take the afrezza the BG rises and stays high while the pancreas is releasing what it has. After it has spiked it takes 2x the afrezza to get it back down. If we take the afrezza before the pancreas has been working hard afrezza will bind to the receptors and get the BG back down for the same carb load. The same carb load should require the same amount of insulin give or take. This is why T1s do carb counting. ... We are discussing different thing here. You are talking about a meal time response, and I am talking about a systemic state. It's a macro vs. micro scope, neither is right or wrong but just different. Carb counting is rather more complicated than that, I wish all carb loads were equal |
|
|
|
Post by uvula on Oct 29, 2022 10:12:27 GMT -5
Short question: Is it possible that t1 and t2 have different causes? Are they different diseases?
|
|
|
|
Post by agedhippie on Oct 30, 2022 8:36:40 GMT -5
Short question: Is it possible that t1 and t2 have different causes? Are they different diseases? Current medical opinion is that they are different diseases. It is quite possible to get both Type 1 and Type 2 diabetes if you are particularly unlucky (someone who got Type 1 in their youth may get Type 2 a few decades later). There are theories linking them, I think the Accelerator Hypothesis is the best fleshed out, but to date no linking mechanism has been found that is considered solid. The problem with Type 2 is that it is a brand rather than a disease. Type 2 for the medical world is, with a couple of exceptions, any instance of diabetes that isn't auto-immune related (hence LADA aka Type 1.5 is considered a Type 1 since it involves GAD65). This means that Type 2 covers a lot of ground and probably origins. The only consistent seems to be the genetic aspect, and that is compounded by needing environmental triggers. |
|
|
|
Post by sayhey24 on Oct 30, 2022 8:40:03 GMT -5
To address your statement "To be clear here; insulin, Afrezza or otherwise does not reduce your systemic insulin resistance" - think about what we can demonstrate. With the exact same carb load if we wait to take the afrezza the BG rises and stays high while the pancreas is releasing what it has. After it has spiked it takes 2x the afrezza to get it back down. If we take the afrezza before the pancreas has been working hard afrezza will bind to the receptors and get the BG back down for the same carb load. The same carb load should require the same amount of insulin give or take. This is why T1s do carb counting. ... We are discussing different thing here. You are talking about a meal time response, and I am talking about a systemic state. It's a macro vs. micro scope, neither is right or wrong but just different. Carb counting is rather more complicated than that, I wish all carb loads were equal OK - point me to some research papers on what you are talking about. What I am talking about is insulin resistance after post prandial response by the pancreas with T2s. The longer you let the pancreas try and get the blood sugar down the more afrezza you need. This is basically the feedback diagram the Wensveens have in their paper. Its also interesting in that if you stop the spike with afrezza and get the PWD back to a non-diabetic baseline over several months it seems to take less afrezza to get the same response. Maybe this is what Al Mann was seeing and why he talked about reversing the condition. Al didn't spend $1B without research backing it up. I still wonder what was in Dave Kendall's "Nuggets of Gold". uvula - No one is sure what causes either T1 or T2 but we do know people react different to the same virus - just look at Covid. We also know its not specifically genetic as numerous studies have been done with identical twins. Is the root cause viral based? I vote yes but no one is 100% sure. Could the same virus cause minimal beta cell loss in some people and nearly 100% in others - I would think yes just as covid killed some people while others never even knew they had it. Its also important to remember while we say T1 and T2 diabetes is really on a spectrum. We also know from lab tests numerous viruses have been able to infect the beta cells. Covid is just one of them. It is also interesting that some people have reported that they have built up an immunity to afrezza after a period of time after it worked great. There is a lot going on in the body and how a person's immune system works and reacts. |
|
|
|
Post by agedhippie on Oct 30, 2022 8:49:13 GMT -5
technical explanations come down to genetics. identified 120 genes that they thought were involved in Type 2 diabetes. If that is the case, explain this? Bariatric (Weight-Loss) Surgery for Treating Diabetes Weight-loss surgery, also called bariatric surgery, can be done in minimally invasive ways and can be used to treat Type 2 diabetes. The surgery treats diabetes by controlling how much sugar is in the blood. One type of surgery is called the duodenal switch. my.clevelandclinic.org/health/treatments/21153-bariatric-weight-loss-surgery-for-treating-diabetes Foods that are high in fats and carbohydrates increases fatty acids in the blood and lipid (fat) build-up in the liver and muscles. This increases insulin resistance and inflammation. Over time, the pancreas stops making enough insulin. ... You can compensate for an issue mechanically or with drugs. The duodenum switch is a mechanical fix as it physically obstructs food absorption. A common part of Type 2 is a broken lipids metabolism (the Syndrome X triad of lipids, glucose, and blood pressure) so stopping food from being absorbed means that the food has less impact. This can also be dealt with by drugs and that is what GLP-1 drugs do (earlier in this thread I posted a GLP-1 graphic that showed the GLP-1 interaction). |
|
|
|
Post by peppy on Oct 30, 2022 9:26:09 GMT -5
technical explanations come down to genetics. identified 120 genes that they thought were involved in Type 2 diabetes. If that is the case, explain this? Bariatric (Weight-Loss) Surgery for Treating Diabetes Weight-loss surgery, also called bariatric surgery, can be done in minimally invasive ways and can be used to treat Type 2 diabetes. The surgery treats diabetes by controlling how much sugar is in the blood. One type of surgery is called the duodenal switch. my.clevelandclinic.org/health/treatments/21153-bariatric-weight-loss-surgery-for-treating-diabetes Foods that are high in fats and carbohydrates increases fatty acids in the blood and lipid (fat) build-up in the liver and muscles. This increases insulin resistance and inflammation. Over time, the pancreas stops making enough insulin. ... You can compensate for an issue mechanically or with drugs. The duodenum switch is a mechanical fix as it physically obstructs food absorption. A common part of Type 2 is a broken lipids metabolism (the Syndrome X triad of lipids, glucose, and blood pressure) so stopping food from being absorbed means that the food has less impact. This can also be dealt with by drugs and that is what GLP-1 drugs do (earlier in this thread I posted a GLP-1 graphic that showed the GLP-1 interaction). or it's the lipids. My hair dresser had a sleeve put in 15 years ago, the new stomach does expand over time. While the duodenum switch was pictured, I had never heard of it before, which means nothing, it looks awful. |
|
|
|
Post by prcgorman2 on Oct 30, 2022 9:59:28 GMT -5
You can compensate for an issue mechanically or with drugs. The duodenum switch is a mechanical fix as it physically obstructs food absorption. A common part of Type 2 is a broken lipids metabolism (the Syndrome X triad of lipids, glucose, and blood pressure) so stopping food from being absorbed means that the food has less impact. This can also be dealt with by drugs and that is what GLP-1 drugs do (earlier in this thread I posted a GLP-1 graphic that showed the GLP-1 interaction). or it's the lipids. My hair dresser had a sleeve put in 15 years ago, the new stomach does expand over time. While the duodenum switch was pictured, I had never heard of it before, which means nothing, it looks awful. Doctors and surgeons never cease to amaze at the Frankensteinian things they will do. On the people are fatter chart, nobody speculated at the reasons. Are Americans just stupid and lazy and therefore fat? And in the context of the chart, now more stupid, more lazy, and therefore more obese? I’ve known some brilliant fat people so I’m not sure there is a direct correlation between inteligence and weight gain. And those anecdotal examples were also not lazy. Far from it. The work they did is what got them recognized as brilliant. If there is a systemic issue with Americans causing increasing levels of obesity and diabetes, I would put it on stress. My oldest loses her appetite when stress levels increase significantly and she becomes thin. My youngest and I are the opposite. Small sample size, but it does make me wonder. Are people more likely to eat more when they’re stressed? And do they fix themselves a salad, or reach for the Doritos? I think there are cravings for salty and sweet foods moreso than vegetables. |
|







