|
|
Post by agedhippie on Jun 24, 2023 7:26:26 GMT -5
Why are they not good? This seems pretty great and the reason for the large study for 2 hour ppg control. ... Did you look at the part 2 graph? It's pretty obvious what the problem is. The HbA1c drop for TS + Tresiba and TS + AID is the same so they are basically equivalent. The drop for the AID pump alone is larger meaning that day to day the AID pump used alone outperforms the other two. I would have expected TS + AID to outperform TS + Tresiba if the idea that the Afrezza weakness in earlier trials was due primarily to the basal insulin, but that didn't happen. That's before we consider the differing starting points. There is a reason why Mannkind always chose the 2 hour PPG. It's because at 3 hours there is no difference, and beyond that RAA is better. This is why things like the HbA1c results are taken more seriously than 2 hr PPG as there is decades of data directly relating HbA1c to complications. This is the chart from the Mannkind website: 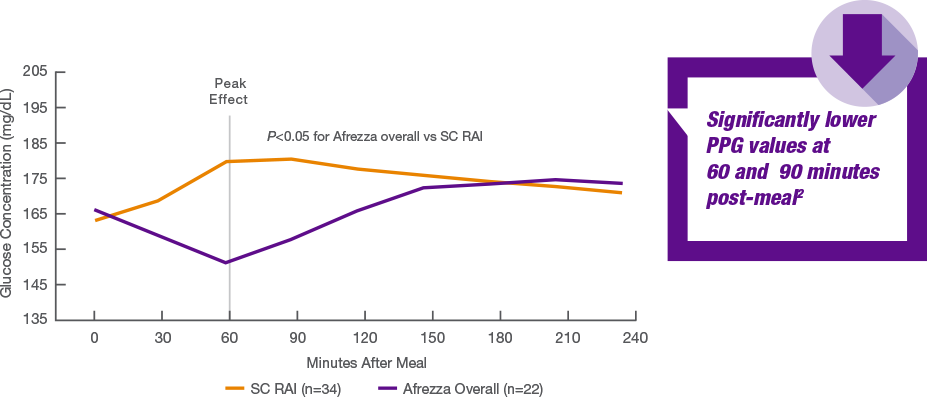 |
|
|
|
Post by sayhey24 on Jun 24, 2023 7:53:02 GMT -5
Why are they not good? This seems pretty great and the reason for the large study for 2 hour ppg control. ... Did you look at the part 2 graph? It's pretty obvious what the problem is. The HbA1c drop for TS + Tresiba and TS + AID is the same so they are basically equivalent. The drop for the AID pump alone is larger meaning that day to day the AID pump used alone outperforms the other two. I would have expected TS + AID to outperform TS + Tresiba if the idea that the Afrezza weakness in earlier trials was due primarily to the basal insulin, but that didn't happen. That's before we consider the differing starting points. There is a reason why Mannkind always chose the 2 hour PPG. It's because at 3 hours there is no difference, and beyond that RAA is better. This is why things like the HbA1c results are taken more seriously than 2 hr PPG as there is decades of data directly relating HbA1c to complications. This is the chart from the Mannkind website: OK butt the issue is not A1c nor is it TIR as currently defined. Its post prandial control. Its about getting back under 140 in 2 hours in the best case. This is why I think Irl Hirsch will be focusing on 2 hour PPG in the study and working to redefine things. The thing is only afrezza can do this so he has his work cut out for him. As we all know A1C is an average like average miles per hour on a trip. The 2 hour PPG is like going through a 45mph area at 65 and getting a ticket. |
|
|
|
Post by agedhippie on Jun 24, 2023 8:04:14 GMT -5
OK butt the issue is not A1c nor is it TIR as currently defined. Its post prandial control. Its about getting back under 140 in 2 hours in the best case. This is why I think Irl Hirsch will be focusing on 2 hour PPG in the study and working to redefine things. The thing is only afrezza can do this so he has his work cut out for him. As we all know A1C is an average like average miles per hour on a trip. The 2 hour PPG is like going through a 45mph area at 65 and getting a ticket. Let's have a look at the trial filing: Primary Outcome Measures :
Change in HbA1c [ Time Frame: 90 days ]
Change in glycated hemoglobin (HbA1c) from baseline to end of study
So actually the issue is A1c.  Interestingly one of the secondary outcome measures is TIR but they don't seem to be talking about that. |
|
|
|
Post by prcgorman2 on Jun 24, 2023 10:56:25 GMT -5
Do you assume releasing news guarantees increases in stock price?
Sounds like your mood could improve if you bought LQDA. Go for it. Best of luck, sincerely. Won't knock your investing choices. Thundersnow, please be polite and thank gorman for his investing and emotional advice. It’s phenomenal! 😅 Moderators, these posts are off-topic so apologies in advance. Do what you think is right. @cretin - Have you ever had to take a pet to the vet to end it’s unreieved suffering? It is an awful experience, but only if you have empathy. The example is poor because an unknown investor is neither a pet nor a close personal friend, but if you have empathy you can’t help notice suffering. If you study psychology, a hallmark of a sociopath is their lack of empathy. You can mock me and gaslight me but you can’t say I don’t have empathy. I’ve never tried to study your posts to detect whether you have empathy, and won’t bother to start now. If you tried to show some, I know my poor outlook would want to assume it was disingenuous and fulsome. My apologies. |
|
|
|
Post by letitride on Jun 24, 2023 11:58:25 GMT -5
What I find interesting is all 3 groups showed an almost equal drop in HbA1c at 90 days was this due to controlled meals like in part1 ?
|
|
|
|
Post by agedhippie on Jun 24, 2023 13:00:48 GMT -5
What I find interesting is all 3 groups showed an almost equal drop in HbA1c at 90 days was this due to controlled meals like in part1 ? It's not unusual in a trial. People tend to be more careful, and also there is a lot more follow up (nagging) than you get from the normal medical staff because they want to make sure you are following the treatment as described. This is one of the reasons why having a reference arm is so important because you want to be sure the improvement is due to the treatment and not just the management protocol. It's also why real world numbers where there are not an army of trial managers standing over people are important. |
|
|
|
ADA 2023
Jun 24, 2023 22:34:49 GMT -5
via mobile
Post by cretin11 on Jun 24, 2023 22:34:49 GMT -5
Thundersnow, please be polite and thank gorman for his investing and emotional advice. It’s phenomenal! 😅 Moderators, these posts are off-topic so apologies in advance. Do what you think is right. @cretin - Have you ever had to take a pet to the vet to end it’s unreieved suffering? It is an awful experience, but only if you have empathy. The example is poor because an unknown investor is neither a pet nor a close personal friend, but if you have empathy you can’t help notice suffering. If you study psychology, a hallmark of a sociopath is their lack of empathy. You can mock me and gaslight me but you can’t say I don’t have empathy. I’ve never tried to study your posts to detect whether you have empathy, and won’t bother to start now. If you tried to show some, I know my poor outlook would want to assume it was disingenuous and fulsome. My apologies. Apology accepted, your outlook may indeed be poor, as was the weird example (attempted analogy?) - but you try very hard and that I can appreciate. Friendly suggestion: don’t presume to tell people how they should invest, nobody is looking for that. If you have empathy you’ll understand! 👍🏼 |
|
|
|
Post by sayhey24 on Jun 25, 2023 6:07:09 GMT -5
OK butt the issue is not A1c nor is it TIR as currently defined. Its post prandial control. Its about getting back under 140 in 2 hours in the best case. This is why I think Irl Hirsch will be focusing on 2 hour PPG in the study and working to redefine things. The thing is only afrezza can do this so he has his work cut out for him. As we all know A1C is an average like average miles per hour on a trip. The 2 hour PPG is like going through a 45mph area at 65 and getting a ticket. Let's have a look at the trial filing: Primary Outcome Measures :
Change in HbA1c [ Time Frame: 90 days ]
Change in glycated hemoglobin (HbA1c) from baseline to end of study
So actually the issue is A1c. Interestingly one of the secondary outcome measures is TIR but they don't seem to be talking about that. The take away is nothing is better than afrezza for meal time control. What this shows is afrezza beats the AID for this. Because of its speed of action there is a reduce chance of hypos which allows a reduction in baseline BG. The question is how aggressive can you get with a T1 and of course that will depend on the person. Buts lets say we can get so aggressive we can target 90 with MDI. the obvious question is what is the AID bringing to the party then? If we want the best A1c the answer is the AID with afrezza. If we want pretty great control and no pump hassle the answer is MDI with afrezza. If we want less control but no daily injects the answer is icodec and afrezza. I know there is a huge pump business but most people really don't want to wear them, especially the kids - if they don't need to. With afrezza, they don't need to. This study is saying nothing different than what we have been saying right here on proboards for years. Mike just needs to get the large scale study done. |
|
|
|
Post by agedhippie on Jun 25, 2023 9:34:22 GMT -5
The take away is nothing is better than afrezza for meal time control. What this shows is afrezza beats the AID for this. Because of its speed of action there is a reduce chance of hypos which allows a reduction in baseline BG. The question is how aggressive can you get with a T1 and of course that will depend on the person. Buts lets say we can get so aggressive we can target 90 with MDI. the obvious question is what is the AID bringing to the party then? If we want the best A1c the answer is the AID with afrezza. If we want pretty great control and no pump hassle the answer is MDI with afrezza. If we want less control but no daily injects the answer is icodec and afrezza. I know there is a huge pump business but most people really don't want to wear them, especially the kids - if they don't need to. With afrezza, they don't need to. This study is saying nothing different than what we have been saying right here on proboards for years. Mike just needs to get the large scale study done. Look at the chart again. If you are looking at the first two hours Afrezza is greatly superior, if you are looking at three hours and further then RAA is superior. Of course you can compensate by taking a second Afrezza dose but now you are taking insulin twice as often as you would with RAA. Maybe you can be aggressive with Afrezza and target 90 with MDI, maybe you can do the same with an AID pump. Until the outcomes are proven in a trial it's all maybes on both sides. Lol. The chart in the paper from The Afrezza ABC trial quite clearly shows that if you want the lowest A1c then you should use an AID pump alone. The gradient of reduction for the AID pumps is steeper than either of the Afrezza options, either AID for basal, or Tresiba. So people don't have to go and dig through the ADA presentations here is the chart:  What matters here is the gradient since that is the amount of reduction in absolute terms from start to finish, the steeper the gradient the better. Two things stand out from this; Using Afrezza will reduce your A1c (no surprise there for us), and that it underperforms the control arm which is just the pump. Actually this is not a trial I would think MNKD should do since the study is not good. The whole point of studies is to pick good trial subjects and avoid bad ones. |
|
|
|
Post by prcgorman2 on Jun 25, 2023 14:13:31 GMT -5
Moderators, these posts are off-topic so apologies in advance. Do what you think is right. @cretin - Have you ever had to take a pet to the vet to end it’s unreieved suffering? It is an awful experience, but only if you have empathy. The example is poor because an unknown investor is neither a pet nor a close personal friend, but if you have empathy you can’t help notice suffering. If you study psychology, a hallmark of a sociopath is their lack of empathy. You can mock me and gaslight me but you can’t say I don’t have empathy. I’ve never tried to study your posts to detect whether you have empathy, and won’t bother to start now. If you tried to show some, I know my poor outlook would want to assume it was disingenuous and fulsome. My apologies. Apology accepted, your outlook may indeed be poor, as was the weird example (attempted analogy?) - but you try very hard and that I can appreciate. Friendly suggestion: don’t presume to tell people how they should invest, nobody is looking for that. If you have empathy you’ll understand! 👍🏼 I can’t accept your apology because it is the same as mine - imaginary. I don’t presume to tell people how they should invest. Encouraging someone to invest in a stock they think is doing well or at least better than MNKD is not telling them to do anything. It’s called being supportive. |
|
|
|
Post by lennymnkd on Jun 25, 2023 14:44:52 GMT -5
If we want less control but no daily injects the answer is icodec and afrezza.
How about icodec Afrezza plus a CGM FOR BETTER CONTROL…
|
|
|
|
Post by agedhippie on Jun 25, 2023 15:31:45 GMT -5
If we want less control but no daily injects the answer is icodec and afrezza. How about icodec Afrezza plus a CGM FOR BETTER CONTROL… I would always advocate for a CGM because you need to make informed decisions, even if the decision is that you are not going to ignore a high for the moment. It's letting you take control of your diabetes. Mannkind used CGMs in the ABC trial, but they haven't published those results. I don't really see why Icodec would give significantly better control than Tresiba. The problem always used to be that Lantus wore off in less than a day so you ended up having to split dose, Toujeo and Tresiba both last over a day so that is fixed. The reason the market thinks Icodec could be a big deal is because T2 diabetics on basal could inject weekly rather than daily which would reduce skipped doses (T1 diabetics don't have the option to skip, but the option to dose weekly is welcome!) |
|
|
|
Post by sayhey24 on Jun 26, 2023 5:49:00 GMT -5
The take away is nothing is better than afrezza for meal time control. What this shows is afrezza beats the AID for this. Because of its speed of action there is a reduce chance of hypos which allows a reduction in baseline BG. The question is how aggressive can you get with a T1 and of course that will depend on the person. Buts lets say we can get so aggressive we can target 90 with MDI. the obvious question is what is the AID bringing to the party then? If we want the best A1c the answer is the AID with afrezza. If we want pretty great control and no pump hassle the answer is MDI with afrezza. If we want less control but no daily injects the answer is icodec and afrezza. I know there is a huge pump business but most people really don't want to wear them, especially the kids - if they don't need to. With afrezza, they don't need to. This study is saying nothing different than what we have been saying right here on proboards for years. Mike just needs to get the large scale study done. Look at the chart again. If you are looking at the first two hours Afrezza is greatly superior, if you are looking at three hours and further then RAA is superior. Of course you can compensate by taking a second Afrezza dose but now you are taking insulin twice as often as you would with RAA. Maybe you can be aggressive with Afrezza and target 90 with MDI, maybe you can do the same with an AID pump. Until the outcomes are proven in a trial it's all maybes on both sides. Lol. The chart in the paper from The Afrezza ABC trial quite clearly shows that if you want the lowest A1c then you should use an AID pump alone. The gradient of reduction for the AID pumps is steeper than either of the Afrezza options, either AID for basal, or Tresiba. So people don't have to go and dig through the ADA presentations here is the chart: What matters here is the gradient since that is the amount of reduction in absolute terms from start to finish, the steeper the gradient the better. Two things stand out from this; Using Afrezza will reduce your A1c (no surprise there for us), and that it underperforms the control arm which is just the pump. Actually this is not a trial I would think MNKD should do since the study is not good. The whole point of studies is to pick good trial subjects and avoid bad ones. If you want control post 2 hours you don't want a prandial. The non-diabetic within two hours should be back to baseline. For all diabetics the goal should be sub-140 in 2 hours. If you want to argue the RAA is better than afrezza after 2 hours what I would say is your RAA sucks. It should be out of your system in 2 hours. This is the advantage of the AID. Its a post 2 hour tool. The whole point of the study is nothing beats afrezza for meal time control. Its also provide a great alternative for T1s who want to ditch the pump but who still want great control. |
|
|
|
Post by sayhey24 on Jun 26, 2023 5:51:06 GMT -5
If we want less control but no daily injects the answer is icodec and afrezza. How about icodec Afrezza plus a CGM FOR BETTER CONTROL… For T1s I am always assuming they are using a CGM. If they are not, well, they are probably not too worried about great control nor hypos. |
|
|
|
Post by agedhippie on Jun 26, 2023 6:56:49 GMT -5
If you want control post 2 hours you don't want a prandial. The non-diabetic within two hours should be back to baseline. For all diabetics the goal should be sub-140 in 2 hours. If you want to argue the RAA is better than afrezza after 2 hours what I would say is your RAA sucks. It should be out of your system in 2 hours. This is the advantage of the AID. Its a post 2 hour tool. The whole point of the study is nothing beats afrezza for meal time control. Its also provide a great alternative for T1s who want to ditch the pump but who still want great control. I'm not the one saying RAA is better after the two hour mark Mannkind is saying it, that's was a link to a chart on their web site. Afrezza is not getting you back to 140 in two hours, it's leaving you at about 170. It would be interesting to see what the chart looks like for the following two hours but understandably they don't seem to be in a hurry to show that. At the end of the day the primary outcome measurement they chose was change in A1c, and the best result came from using an AID pump and not adding Afrezza. Notice that they haven't published TIR although they have that data. |
|







