|
|
Post by BD on Oct 2, 2024 20:28:33 GMT -5
The inclusion criteria for the trial says, " MDI, an AID system, or an insulin pump without automation. The PR says, "multiple daily injections (MDI), an automated insulin delivery system, (AID) or a pump without automation." I think it's safe to say automated pump means AID. You are correct though, even dumb pumps some automation because they change basal rates on a schedule you give it. Blah blah blah. Did the peak times and the out of system times change on these Rapid Acting Subq insulins?  Hard to get the blood glucose control the correct use of Afrezza gives. You know, you keep saying "blah blah blah" at people, they might start taking it personally... |
|
|
|
Post by peppy on Oct 2, 2024 20:58:24 GMT -5
Blah blah blah. Did the peak times and the out of system times change on these Rapid Acting Subq insulins? Hard to get the blood glucose control the correct use of Afrezza gives. You know, you keep saying "blah blah blah" at people, they might start taking it personally... aged and I know each other. aged uses multiple daily injection using a pen. You do know that peak on the RAA's is @ 90 mins and out of system 5 to 6 hours correct? Afrezza peak 35 mins out of system 90 mins for a 4 unit cartridge. Subq pumps can not make RAA's work faster. So what happens is the type one goes high and then low using subq rapid acting insulin. A low A1c the lows average the highs. Aged points out a no carb diet blunts highs if people go that route. Don't get me wrong, it is the delivery route that makes RAA's so slow. Put the insulin in an IV bag and run it into a human being IV, it works fast. Better control the amount and rate. . |
|
|
|
Post by ktim on Oct 3, 2024 1:40:40 GMT -5
That's why AID pumps have predictive algorithms for insulin action. And, as Al Mann said there was no algorithm he could write which could over come the speed of the RAA . Now Al could write one hell of an algorithm but as he said the RAA was just too damn slow. Long story short, arfezza kicked the ass of the AID just as Al knew it would. The ATTD should be fun. We will get to see the Inhale-3 details and the kids data. Carol Levy jumped on the train just in time. Seems like she would have had a bit more time to jump on the train, since detailed results being held back until March. BTW... the A1C reduction was 16 basis points for one arm and 23 for the other. It undoubtedly was less compared to AID since AIDs are definitely better than the other 2 usual care options. Is that really an "ass kick" in your mind? If you are expecting a split out off AID in March and that it would be something awesome for Afrezza, I just don't see how that could be mathematically possible given other data about how much AIDs outperform manual MDI. Though I'm sure the standard argument could be made that it was the fault of the study design, study administration or patients behaving too much like humans (less than perfect). |
|
|
|
Post by letitride on Oct 3, 2024 4:55:29 GMT -5
It is apparent to me that if you live your life on a critically controlled diet hooked up to an AID you can circumvent the need for afrezza. As a critical care doctor in an ICU told me upon seeing the coke challenge I wouldnt want to try that here hooked up to an IV. And as a type 1 ER doctor told me afrezza changed my life. So I have concluded from these conversations AID is great if you live your life like an android but if you want to live your life more human afrezza has your back.
|
|
|
|
Post by prcgorman2 on Oct 3, 2024 6:31:50 GMT -5
And, as Al Mann said there was no algorithm he could write which could over come the speed of the RAA . Now Al could write one hell of an algorithm but as he said the RAA was just too damn slow. Long story short, arfezza kicked the ass of the AID just as Al knew it would. The ATTD should be fun. We will get to see the Inhale-3 details and the kids data. Carol Levy jumped on the train just in time. Seems like she would have had a bit more time to jump on the train, since detailed results being held back until March. BTW... the A1C reduction was 16 basis points for one arm and 23 for the other. It undoubtedly was less compared to AID since AIDs are definitely better than the other 2 usual care options. Is that really an "ass kick" in your mind? If you are expecting a split out off AID in March and that it would be something awesome for Afrezza, I just don't see how that could be mathematically possible given other data about how much AIDs outperform manual MDI. Though I'm sure the standard argument could be made that it was the fault of the study design, study administration or patients behaving too much like humans (less than perfect). It must be very difficult to be a person with diabetes. A constant fight. It’s like rust. It never sleeps. agedhippie has said the fatigue of dealing with diabetes is what drives the desire for options which reduce the fatigue. Having to more closely monitor blood glucose, estimate dosing of insulin, and taking more doses is moving in the opposite direction of reducing fatigue. In respect of these very understandable attitudes towards diabetes care, an AID may be more convenient and desirable for both the person with diabetes and their doctor. If a large clinical trial demonstrated people with the option to do either preferred Afrezza and had better results in terms of A1C, TIR, comorbidity, SAFETY, and somehow the STEP programs and Prior Authorizations were no longer required and the premium for Afrezza was similar to the premium(?) for AID treatment, maybe we would see a significant improvement in sales of Afrezza. My hunch is that large clinical trial has been done with real live patients, but only as users, not as a formal trial, and the data isn’t available to be colated, analyzed, and presented. So the INHALE-3 trial is the next best thing, but is that enough? |
|
|
|
Post by uvula on Oct 3, 2024 8:03:28 GMT -5
If i could add a little bit to prc's post: I believe that if history was altered and Al Mann discovered Afrezza today, he would not pursue developing it because it would not provide a significant life improving benefit over modern AIDs.
I do not mean to suggest in any way that prc agrees with anything I just wrote. These are just my thoughts that were clarified in my mind while reading prc's post.
|
|
|
|
Post by prcgorman2 on Oct 3, 2024 8:30:05 GMT -5
Being hooked up to a machine 24/7 is not a picnic. It could inhibit a lot of activities. I would (and may get the opportunity as a T2 to) choose Afrezza. But I recognize it is one tool in the toolkit and other tools must be available. Developing a serious cough during flu or other respiratory illness would be an example where a hopefully temporary alternative would be important. I think Afrezza could be that for an AID user too. A temporary alternative to enable freedom from the pump for an activity or just because a break would be welcome.
|
|
|
|
Post by ktim on Oct 3, 2024 8:45:57 GMT -5
It is apparent to me that if you live your life on a critically controlled diet hooked up to an AID you can circumvent the need for afrezza. As a critical care doctor in an ICU told me upon seeing the coke challenge I wouldnt want to try that here hooked up to an IV. And as a type 1 ER doctor told me afrezza changed my life. So I have concluded from these conversations AID is great if you live your life like an android but if you want to live your life more human afrezza has your back. But as some here complained about the 17 week results, some in the Afrezza arm they said should be thrown out of the data because they weren't compliant with follow up doses and thus resulted in worsening numbers having been switched to Afrezza... so there is a bit of regiment (android behavior as you put it) to getting great results with Afrezza that some don't want. I've never had to deal with it, so really don't have a perspective on what I'd prefer. We do know from presentation on 17 week results that it was said by one of the luminaries that Afrezza is a better match for some patients than others (paraphrasing here as I don't remember the exact wording or care enough to track it down, but that was the gist). Sounds like you know you'd definitely prefer Afrezza to an AID if faced with the dilemma. I'd hope that you'd have insurance coverage for your choice, though I suspect that will always require jumping through hoops of preauth. For me personally I eat healthy and balanced meals, likely what you would characterize as a critically controlled diet. I'd never dream of doing a coke challenge even as someone without diabetes... because I want to stay that way. If I ever needed it, I suspect an AID would handle my diet just fine. |
|
|
|
Post by sayhey24 on Oct 3, 2024 14:10:17 GMT -5
If i could add a little bit to prc's post: I believe that if history was altered and Al Mann discovered Afrezza today, he would not pursue developing it because it would not provide a significant life improving benefit over modern AIDs. I do not mean to suggest in any way that prc agrees with anything I just wrote. These are just my thoughts that were clarified in my mind while reading prc's post. Did you know Al Mann invented the CGM and the AID? He was looking for a faster insulin for the CGM controlled pump, aka AID. There are few people alive today which could write a better algorithm for the AID than Al Mann. What I think is you are not fully appreciating afrezza. Al developed it for the T2s. He knew if we got the early diagnosed T2s on afrezza in many cases the progression would be stopped and even reversed. He knew it would have benefit with the T1s but that is not why he invested $1B of his own money. The problem we have is we have not yet addressed the T2 market. GLP1s came along and have shown a significant 1.5 - 2% A1c reduction at the same time MNKD ran out of money. Mike pivoted to the T1s as it was seen as lower hanging fruit. However afrezza is a T2 solution, a near cure. The funny thing is Al got into the diabetes business because he was trying to make a better pacemaker. The cardiac doctor told him he was barking up the wrong tree and that all the people in the ward with heart issues were diabetics. He was told if he wanted to solve the cardiac issue he needs to solve the diabetes. Nothing has changed. The number 1 cause of heart disease is diabetes but Al did find a way to stop T2 progression. I am sure to him that was worth his $B investment. |
|
|
|
Post by uvula on Oct 3, 2024 14:56:27 GMT -5
Sayhey, when I wrote my comment I was thinking about T1 and completely forgot about T2. Thank you for waking me up.
|
|
|
|
Post by sayhey24 on Oct 3, 2024 14:59:27 GMT -5
Seems like she would have had a bit more time to jump on the train, since detailed results being held back until March. BTW... the A1C reduction was 16 basis points for one arm and 23 for the other. It undoubtedly was less compared to AID since AIDs are definitely better than the other 2 usual care options. Is that really an "ass kick" in your mind? If you are expecting a split out off AID in March and that it would be something awesome for Afrezza, I just don't see how that could be mathematically possible given other data about how much AIDs outperform manual MDI. Though I'm sure the standard argument could be made that it was the fault of the study design, study administration or patients behaving too much like humans (less than perfect). It must be very difficult to be a person with diabetes. A constant fight. It’s like rust. It never sleeps. agedhippie has said the fatigue of dealing with diabetes is what drives the desire for options which reduce the fatigue. Having to more closely monitor blood glucose, estimate dosing of insulin, and taking more doses is moving in the opposite direction of reducing fatigue. In respect of these very understandable attitudes towards diabetes care, an AID may be more convenient and desirable for both the person with diabetes and their doctor. If a large clinical trial demonstrated people with the option to do either preferred Afrezza and had better results in terms of A1C, TIR, comorbidity, SAFETY, and somehow the STEP programs and Prior Authorizations were no longer required and the premium for Afrezza was similar to the premium(?) for AID treatment, maybe we would see a significant improvement in sales of Afrezza. My hunch is that large clinical trial has been done with real live patients, but only as users, not as a formal trial, and the data isn’t available to be colated, analyzed, and presented. So the INHALE-3 trial is the next best thing, but is that enough? The three issues remain; label; SoC; cost. Inhale-3 when combined with the kids should be enough to provide changes to the SoC and then hopefully insurance follows to address cost. Lets hope the plan works. If it does then happy days are here. |
|
|
|
Post by sayhey24 on Oct 3, 2024 15:17:08 GMT -5
Sayhey, when I wrote my comment I was thinking about T1 and completely forgot about T2. Thank you for waking me up. NP - MNKD has been a company with a cult following very much like Apple in their early days when Bill Gates lent them money to kept them in business. Apple had Bill Gates and MNKD has Martine. Many of our cult followers are T1s as they know much more about diabetes and insulin. They then became the low hanging fruit for afrezza. The T2s not so much. They go to their doctor and get a pill which fails and then they get another and now a GLP1 which over time fails too. Most don't even test their BG yet most over time progress and incur heart disease and then die from a heart attack. The T2s are nearly 100% relying on their doctors who don't know. All they know is follow the SoC our great "treat to fail" protocol. There was a pretty big and new study I saw the other week about heart disease and cholesterol and BG. They were stunned that heart disease was less about cholesterol and more about BG control. That doctor told Al that many years ago that it was about BG control which started him down this diabetes path. |
|
|
|
Post by agedhippie on Oct 3, 2024 16:40:38 GMT -5
... You do know that peak on the RAA's is @ 90 mins and out of system 5 to 6 hours correct? Afrezza peak 35 mins out of system 90 mins for a 4 unit cartridge. Subq pumps can not make RAA's work faster. So what happens is the type one goes high and then low using subq rapid acting insulin. A low A1c the lows average the highs. Aged points out a no carb diet blunts highs if people go that route. ... There is some confusing around how AID pumps work that make the behavior of RAA is a lot less important than it appears. Before we start I agree that Afrezza is faster than RAA, even with what I am about to describe. I will summarize about AID pumps here because there is a ton of text and some people will not want to read it all. - Pumps use the same approach as CGMs and predict where your levels are going and use that to adjust the rate of flow - They use the long tail of RAA to have active insulin on-board when they need it. This isn't as fast as Afrezza, but it's faster that a new dose of RAA. - Pumps get better results if you don't mess with them and let them do their stuff. - Real world pump results for the Medtronics 780G have 78% TIR and 56% of that between 140 and 70. That's across 7,500 people. - If you want to use MDI then Afrezza will outperform RAA. - Most important of all is that numbers are not the only reason people pick an option. On to the details.... When you take RAA there is that slow onset and long tail. The aim becomes to reduce the onset and you do that by having active insulin on-hand - that long tail. I do this manually by taking more insulin than I need because I know I am going to eat again, and when I do that eat that excess acts as a prebolus giving me active insulin that can start going to work without such a long onset. If that prebolus is not going to be enough I can take a dose for the meal time that matches the carbs - I stack the insulin. The prebolus now deals with some of the carbs, but the stacked insulin is needed for the balance. The down side to this is that I had better eat or I am going low. What AID pumps do is similar. They only use RAA and simulate basal the same way your body does, by continuously feeding insulin (RAA in this case) to offset the basal glucose output. The pump knows what the PK/PD curves look like for a given insulin and uses that to predict where your levels will be. Remember that mother complaining that Levemir was going away and her daughter needed to be able to reduce her basal sometimes? This is what the pump is doing. It's a longer range version of what the CGM does with interstitial fluid predicting where you really are from where you were 20 minutes ago. When you eat the AID assigns part of the insulin it's using as basal to deal with the food. It's not going to be enough, but it's immediately active - think first phase response. It has to replace that insulin because it already had a purpose, dealing with your basal glucose, and it needs to bolus for the balance of the food. That takes time and is why Afrezza gets better results. There is no need for a follow up though because the pump is already watching and making corrections in real time. How good is the pump? 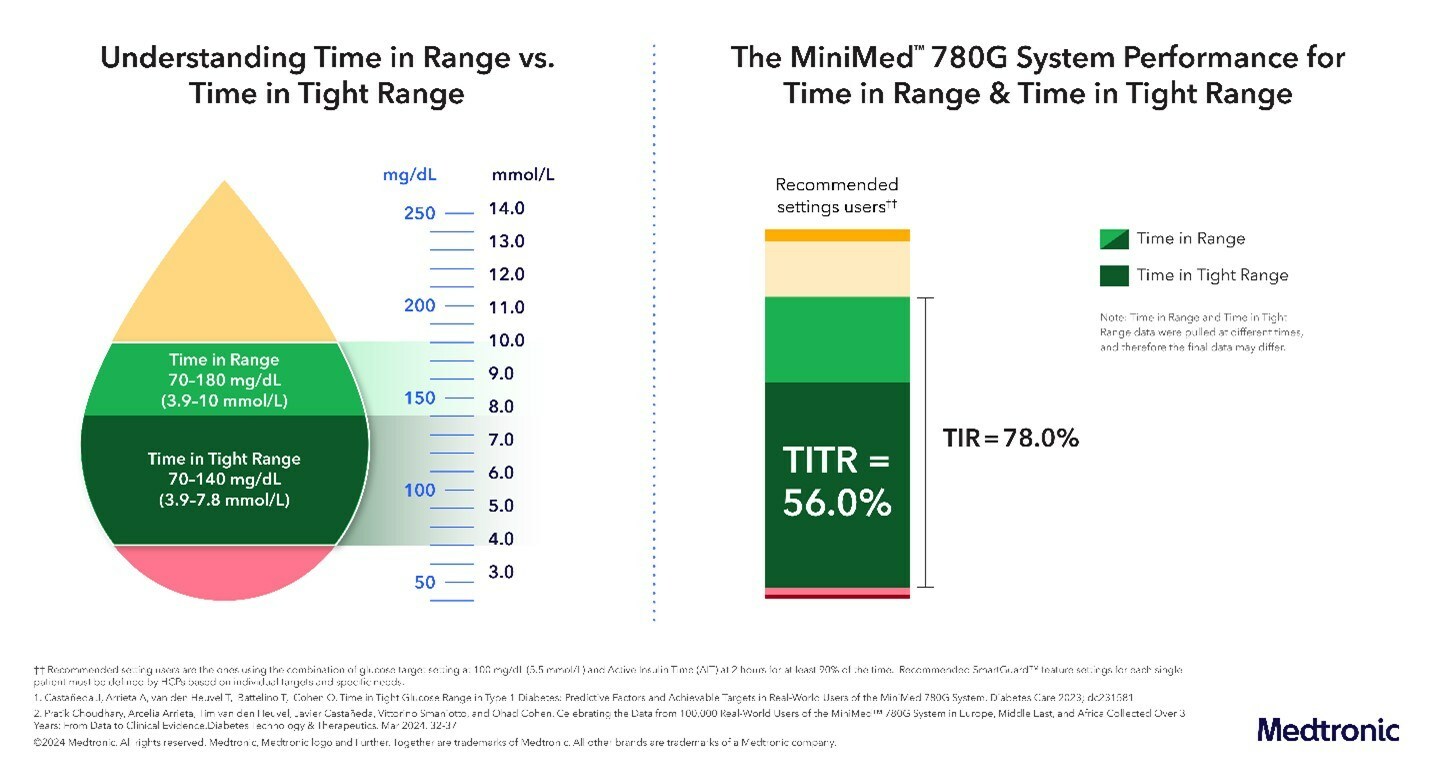 This is an infographic from Medtronics showing TIR and TTIR for their 780G AID pump users (7,500 people) so no cherry picking. The algorithms in these pumps are that good. Can they beat Afrezza for a meal time dose? No. But what is important is the system and not the components. Afrezza will deliver an overall inferior result from the data we have because there are humans in the loop who mess up (forget to dose, underdose, just eat without dosing, ignore the follow up dose, etc.), and because the basal rate is fixed so if your levels start to rising in the middle of the night you are out of luck. The pump does screw up, it just screws up less, and it's adjusting every five minutes which you cannot do manually. Where does this go? Some of the DIY AID pumps can use t-shirt sizing and unannounced snacks. You just tell it if the meal is small medium, or large and the pump doses and adjusts to deal with it. If you only eat a few carbs like a snack you don't even need to tell it, it spots the rise and deals with it. This is the next step with pumps and that might just be enough to get me to bite the bullet and use on. All of this is talking about AID pumps. If you are MDI and using RAA then you inherit all the issues I talked about with humans and Afrezza will easily out-perform RAA. The decision then is which you prefer and why. Deciding what and why you want to use an option is not predicated purely on performance (or I would be on an AID pump already) but rather what fits you, the diabetic, best and is sustainable. As an example, I am on MDI using RAA which is probably the least optimal solution, but I am comfortable with it and it fits my lifestyle so I am not in a hurry to change. I would like to congratulate anyone who finished this wall of text! |
|
|
|
Post by peppy on Oct 3, 2024 17:01:29 GMT -5
|
|
|
|
Post by ktim on Oct 3, 2024 19:36:11 GMT -5
Sayhey, when I wrote my comment I was thinking about T1 and completely forgot about T2. Thank you for waking me up. NP - MNKD has been a company with a cult following very much like Apple in their early days when Bill Gates lent them money to kept them in business. Apple had Bill Gates and MNKD has Martine. Many of our cult followers are T1s as they know much more about diabetes and insulin. They then became the low hanging fruit for afrezza. The T2s not so much. They go to their doctor and get a pill which fails and then they get another and now a GLP1 which over time fails too. Most don't even test their BG yet most over time progress and incur heart disease and then die from a heart attack. The T2s are nearly 100% relying on their doctors who don't know. All they know is follow the SoC our great "treat to fail" protocol. There was a pretty big and new study I saw the other week about heart disease and cholesterol and BG. They were stunned that heart disease was less about cholesterol and more about BG control. That doctor told Al that many years ago that it was about BG control which started him down this diabetes path. This isn't considered definitive but I certainly wouldn't class this as GLP-1s being a treat to fail protocol. "Low quality of evidence revealed that GLP-1RAs significantly increased the incidence of prediabetes reversion to the normoglycemic state [RR = 1.76, 95% CI (1.45, 2.13), P < 0.00001] and moderate quality of evidence showed that GLP-1RAs significantly prevented new-onset diabetes [RR = 0.28, 95% CI (0.19, 0.43)" I don't think early use of insulin (inhaled or otherwise) could make any stronger claims regarding halting or reversing. |
|










