|
|
Post by markado on Feb 22, 2023 13:02:38 GMT -5
It could very well be, maybe is NVO. Big Pharma is known for protecting franchises, but also for purposeful self cannibalization and replacement. For them, it's all about big numbers (of patients / Rxs), consumable solutions, cost and projectable profit. If someone sat down to see what share of the market inhaled insulin solutions or glycemic control solutions could Garner over injectables, and the associated ease of use, adoption, and profit, it would be easy to see the future option and net present value of Afrezza in bigger hands than mnkd's. Few longs would be disappointed in a buyout of Afrezza associated with manufacturing revenues and the possibility/promise of additional collaborations for diabetes management down the road (if not immediately). Make it so, Mike!
|
|
|
|
Post by Chris-C on Feb 22, 2023 13:34:26 GMT -5
Its all about the highest bidder.  ... And we've got 27 billion. Do I hear 28? From your lips to God's ears... Now I'm getting nervous. Too much promising news regarding MNKD. It's like a starving/thirsty guy in the desert who discovers fresh water and then worries that it's a mirage or poisoned with toxic contaminants.  |
|
|
|
Post by agedhippie on Feb 22, 2023 16:36:16 GMT -5
Here comes your favorite wet blanket I have no idea why anyone thinks this is a surprise unless they don't understand how AID pumps work. TL;DR You have bolused for the meal and hence have insulin onboard so the pump (correctly) will not adjust the basal rate. Therefore the result should be the same as for STAT - you are looking at RAA bolus vs. Afrezza and already STAT told us what that outcome will be. Longer version You are looking at a maximum of 120 minutes. We already know from the STAT results that what the 120 minute readings will be: 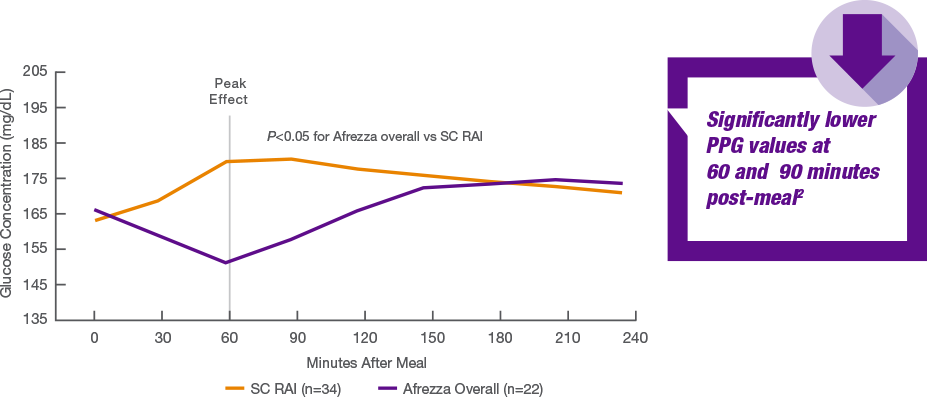 Why does anyone think this is going to different for an AID pump over Tresiba? The AID pump provides basal via RAA, and because the pump knows you have bolused it know there is insulin onboard to cover the food so it's not going to change the basal RAA and you get a flat basal curve, just like you would with Tresiba. This is a definitely not going to move the endos. The large scale ABC trial will be interesting, especially the Afrezza with food and pump the rest of the time arm. |
|
|
|
Post by sayhey24 on Feb 22, 2023 17:50:48 GMT -5
I told Mango earlier you would not like this.
I wouldn't say wet blanket I would say your argument is more like a wet noodle. The entire purpose of the AID is to provide better control in the 2 hour period after meals and to attempt to stop the spike to avoid the out of control highs. Tresiba is not doing that. Afrezza is.
The bottom line is afrezza wins big. The question is does the AID provide better control when the PWD is sleeping than a patch pump or Tresiba and if so how much more. We know it loses at mealtime. I think we now know why Lane Desborough is working for MNKD. He just couldn't beat afrezza with his algorithms.
The large scale trial will provide better numbers for afrezza when they properly dose. The food will prove too unpredictable for the algorithm and slow RAA. For afrezza its a simple puff or the liver providing a helping hand.
After 8 years we are finally doing what the doctor at the Adcom did when the FDA review team accused him of cheating because his A1c numbers were to good. He properly dosed. Maybe the AID vendors will now accuse MNKD of cheating?
|
|
|
|
Post by agedhippie on Feb 22, 2023 18:09:29 GMT -5
I told Mango earlier you would not like this. I wouldn't say wet blanket I would say your argument is more like a wet noodle. The entire purpose of the AID is to provide better control in the 2 hour period after meals and to attempt to stop the spike to avoid the out of control highs. Tresiba is not doing that. Afrezza is. ... Did you read what I wrote because you don't seem to understand how AID works. The AID pump did exactly what is should have done which not to change any settings because you had bolused so it had sufficient insulin to cover the carbs. Hence you are replicating that STAT graph. Afrezza starts faster than RAA. That's not exactly news and why no endo will care. As to the AID performance, they understand the concept of insulin on-board. |
|
|
|
Post by sayhey24 on Feb 22, 2023 18:37:42 GMT -5
Of course I read what you wrote but as I said in not so many words - when compared to afrezza the AID sucks. Afrezza kicks ass at the 60minute mark and if they second dosed like the Adcom doctor did the afrezza numbers would have been even better.
What this says - in not so many words is - take the AID and throw it in the trash for mealtime control.
The problem with the STAT study was what Dave Kendall said at the time and that was - bigger trials would follow. They never did. Mike says he has a partner for the "Big" follow-on trial. Maybe tomorrow we get a PR on who it is.
|
|
|
|
Post by neil36 on Feb 23, 2023 13:58:16 GMT -5
www.hcplive.com/view/inhaled-insulin-bests-rapid-acting-insulin-for-post-prandial-glucose-control-in-pilot-studyInhaled Insulin Bests Rapid-Acting Insulin for Post-Prandial Glucose Control in Pilot Study
Feb 23, 2023 Patrick Campbell Data presented at the 16th International Conference on Advanced Technologies & Treatment for Diabetes (ATTD 2023) is providing new insight into the effects of inhaled technosphere insulin when combined with automated insulin delivery (AID) systems for lowering peak glucose levels and post-prandial glucose.1 The study, which was presented by Kevin Kaiserman, MD, a pediatric endocrinologist and Vice President of Medical Affairs in the Endocrine Business Unit for MannKind, returned results indicating inhaled technosphere insulin lowered peak glucose levels 30 minutes faster than injectable rapid-acting insulin delivered through an AID insulin pump and significantly lowered post-prandial glucose from 45-120 minutes after a controlled meal challenge test.1 “We believe inhaled insulin is an important option for those living with type 1 diabetes to reduce their post-prandial glucose in the first 120 minutes,” Kaiserman said.2 “The study revealed a faster and lower peak in glucose that may assist patients in achieving improved glycemic control.” A pilot study of 26 adults with type 1 diabetes already using AID, the trial randomized 21 patients to receive an inhaled insulin dose to cover a standardized meal and 5 patients to the AID control group, which received AID-administered rapid-acting insulin analogue to cover a standardized meal. The ATTD 23, which was a subset analysis of the trial, was designed with the specific intent of examining the efficacy and safety of an ultra-rapid-acting inhaler insulin for the 2 hours proceeding a standard meal.1 Of note, those randomized to techno’s-here insulin achieved an immediate pre-prandial dose of techno’s-here insulin calculated by doubling their usual rapid-acting insulin analogue doses and rounding down to the nearest technosphere insulin dose. The control group received a typical pump bolus up to 15 minutes before the meal. Investigators pointed out self-monitoring of blood glucose was measured using the Ascension Contour meter and timepoints of 0, 15, 30, 45, 60, 90, and 120 minutes relative to the meal.1 Upon analysis, results indicated those randomized to technosphere insulin experienced lower peak glucose levels 30 minutes faster (200 mg/dl at 60 minutes) than their counterparts in the study’s control group (264 mg/dL at 90 minutes). Further analysis demonstrated those randomized to technosphere insulin experienced significantly lower mean post-prandial glucose from 45 to 120 minutes post-meal.1 “We are steadfast in our commitment to addressing the serious unmet need to improve mealtime control for those living with diabetes,” said Michael Castagna, PharmD, Chief Executive Officer of MannKind Corporation.2 “Based on the data collected from this pilot study we intend to move forward with a larger study this year to evaluate how we can reduce the diabetes burden as well as improve a patient’s ability to control their sugars in the first 120 minutes after they eat.” References: Kaiserman K. INHALED INSULIN + AID SAFELY REDUCED GLUCOSE COMPARED TO AID ADMINISTERED RAA FOLLOWING IN-CLINIC MEAL IN PROOF-OF-CONCEPT STUDY DATA SUBSET. Advanced Technologies and Treatments for Diabetes 2023. February 2023. MannKind. Mannkind to give oral presentation on Meal Challenge results from the afrezza® with basal combination (ABC Study) at 16th annual ATTD conference. GlobeNewswire News Room. www.globenewswire.com/news-release/2023/02/22/2612958/29517/en/MannKind-to-Give-Oral-Presentation-on-Meal-Challenge-Results-From-the-Afrezza-With-Basal-Combination-ABC-Study-at-16th-Annual-ATTD-Conference.html. Published February 22, 2023. Accessed February 23, 2023.
|
|
|
|
Post by sayhey24 on Feb 25, 2023 8:09:24 GMT -5
|
|
|
|
Post by agedhippie on Feb 25, 2023 13:20:17 GMT -5
A different link to the same thing: www.liebertpub.com/doi/full/10.1089/dia.2023.2525.abstractsSearch for Mannkind, there is only one hit and that's the one you want. To be clear; this presentation is not the results from ABC, it's just the results from one part of that trial. There is more to come.... |
|
|
|
Post by agedhippie on Feb 25, 2023 13:35:25 GMT -5
... At the 2hr mark there is a really significant difference between TI+AID vs AID alone - about 50mg/dl. Thats surprising to me that AID still had not caught up at 2hrs. I think the difference between this and Dave Kendall's STAT was the dosing and of course help of the AID after 90 minutes. For this they based the afrezza dosing on doubling the RAA dose and rounding down. ... The curve for RAA is well established so the results from the AID are exactly as expected. Since the pump has delivered insulin for the food when the person ate and that insulin is still active the pump is simply maintaining the basal. It's quite possible for the pump to issue more insulin and chase the curve, but now you have all the insulin you need plus an extra dose - that's the sort of stacking that causes hypos as they now would have far to much insulin in your system. |
|
|
|
Post by sayhey24 on Feb 25, 2023 13:37:15 GMT -5
Correct - Mike said they were holding the main data for ADA2023. This is only afrezza with AID and AID without afrezza. This does not include Tresiba. What we can say is the graphs they presented are nothing like the graph you referred to earlier in the thread from STAT. I guess I can also say it makes sense Lance is now working with MNKD. There is no way he can write an alogorithm to beat this. It looks like we have come full circle from 10 years ago and this - www.youtube.com/watch?v=GGgGjtM5ipg |
|
|
|
Post by peppy on Feb 25, 2023 13:40:30 GMT -5
... At the 2hr mark there is a really significant difference between TI+AID vs AID alone - about 50mg/dl. Thats surprising to me that AID still had not caught up at 2hrs. I think the difference between this and Dave Kendall's STAT was the dosing and of course help of the AID after 90 minutes. For this they based the afrezza dosing on doubling the RAA dose and rounding down. ... The curve for RAA is well established so the results from the AID are exactly as expected. Since the pump has delivered insulin for the food when the person ate and that insulin is still active the pump is simply maintaining the basal. It's quite possible for the pump to issue more insulin and chase the curve, but now you have all the insulin you need plus an extra dose - that's the sort of stacking that causes hypos as they now would have far to much insulin in your system.You use a pen. You have control of how much insulin you have on board when. It would seem you prefer control of your own insulin determination. |
|
|
|
Post by sayhey24 on Feb 25, 2023 14:04:25 GMT -5
... At the 2hr mark there is a really significant difference between TI+AID vs AID alone - about 50mg/dl. Thats surprising to me that AID still had not caught up at 2hrs. I think the difference between this and Dave Kendall's STAT was the dosing and of course help of the AID after 90 minutes. For this they based the afrezza dosing on doubling the RAA dose and rounding down. ... The curve for RAA is well established so the results from the AID are exactly as expected. Since the pump has delivered insulin for the food when the person ate and that insulin is still active the pump is simply maintaining the basal. It's quite possible for the pump to issue more insulin and chase the curve, but now you have all the insulin you need plus an extra dose - that's the sort of stacking that causes hypos as they now would have far to much insulin in your system. Aged - you are correct if they stacked with an RAA but that is the beauty of afrezza. At 90minutes its about done and at 2hours its done. If that curve was going up at 90minutes like it may with Tresiba and your STAT graph another puff of afrezza will do it. We will find out in June. This was the doctor's argument at Adcom when he second dosed the afrezza and they accused him of cheating since he did not second dose the RAA users. He said he would have killed his RAA patients. I think the long and short of it is afrezza kicks ass and about the only thing holding it back is more and more big studies and the ability to strong arm the industry to pay attention. |
|
|
|
Post by agedhippie on Feb 25, 2023 15:00:49 GMT -5
Lol. Oh look - it's the Afrezza dose with AID system arm of ABC! There were no commercial AID systems 10 years (their algorithm ran on a laptop!) and you can probably get even better results now. I am interested to see how that single dose at the start of a meal with the AID system covering everything else works. |
|
|
|
Post by agedhippie on Feb 25, 2023 15:18:48 GMT -5
... It's quite possible for the pump to issue more insulin and chase the curve, but now you have all the insulin you need plus an extra dose - that's the sort of stacking that causes hypos as they now would have far to much insulin in your system.You use a pen. You have control of how much insulin you have on board when. It would seem you prefer control of your own insulin determination. Both the pump and I agree - if I have enough insulin onboard to cover the meal I should not take more to chase the curve. TBH though, sometimes I will stack because I know that before my levels drop badly I will have eaten again - think of it as long range pre-bolusing! But just to chase the curve? No. |
|


 ... And we've got 27 billion. Do I hear 28?
... And we've got 27 billion. Do I hear 28?


