|
|
Post by agedhippie on Feb 25, 2023 15:30:34 GMT -5
Correct - Mike said they were holding the main data for ADA2023. This is only afrezza with AID and AID without afrezza. This does not include Tresiba. What we can say is the graphs they presented are nothing like the graph you referred to earlier in the thread from STAT. I guess I can also say it makes sense Lance is now working with MNKD. There is no way he can write an alogorithm to beat this. ... I realized I didn't answer the first part of that post! The graph curves are the same except that they are cut off after 2 hours unlike the STAT graph which ran for five hours. This was using a standardized meal under lab conditions, STAT was real world so the meal were wherever and anything but standardized  You attach way to much importance to Nudge BG performing a consultancy engagement with Mannkind. If you hire an industry expert consultant that doesn't mean they are working with you beyond that engagement (or I am working for a ton of companies!) |
|
|
|
Post by peppy on Feb 25, 2023 15:46:31 GMT -5
You use a pen. You have control of how much insulin you have on board when. It would seem you prefer control of your own insulin determination. Both the pump and I agree - if I have enough insulin onboard to cover the meal I should not take more to chase the curve. TBH though, sometimes I will stack because I know that before my levels drop badly I will have eaten again - think of it as long range pre-bolusing! But just to chase the curve? No. well you have 1 and 1/2 to 2 hours, so..... yep. Peak serum concentrations of insulin lispro occur 30 to 90 minutes after subcutaneous administration. www.aafp.org/pubs/afp/issues/1998/0115/p279.html |
|
|
|
Post by peppy on Feb 25, 2023 15:49:00 GMT -5
Correct - Mike said they were holding the main data for ADA2023. This is only afrezza with AID and AID without afrezza. This does not include Tresiba. What we can say is the graphs they presented are nothing like the graph you referred to earlier in the thread from STAT. I guess I can also say it makes sense Lance is now working with MNKD. There is no way he can write an alogorithm to beat this. ... I realized I didn't answer the first part of that post! The graph curves are the same except that they are cut off after 2 hours unlike the STAT graph which ran for five hours. This was using a standardized meal under lab conditions, STAT was real world so the meal were wherever and anything but standardized You attach way to much importance to Nudge BG performing a consultancy engagement with Mannkind. If you hire an industry expert consultant that doesn't mean they are working with you beyond that engagement (or I am working for a ton of companies!) The stat showed how fearful type ones were to take a follow dose. You know afrezza needs the one hour follow up dose. |
|
|
|
Post by JEvans on Feb 25, 2023 16:01:00 GMT -5
MannKind to Give Oral Presentation on Meal Challenge Results From the Afrezza® With Basal Combination (ABC Study) at 16th Annual ATTD Conference today 2/25/23.
Has any listened to this? I can't locate
|
|
|
|
Post by peppy on Feb 25, 2023 16:32:44 GMT -5
Here comes your favorite wet blanket I have no idea why anyone thinks this is a surprise unless they don't understand how AID pumps work. TL;DR You have bolused for the meal and hence have insulin onboard so the pump (correctly) will not adjust the basal rate. Therefore the result should be the same as for STAT - you are looking at RAA bolus vs. Afrezza and already STAT told us what that outcome will be. Longer version You are looking at a maximum of 120 minutes. We already know from the STAT results that what the 120 minute readings will be: 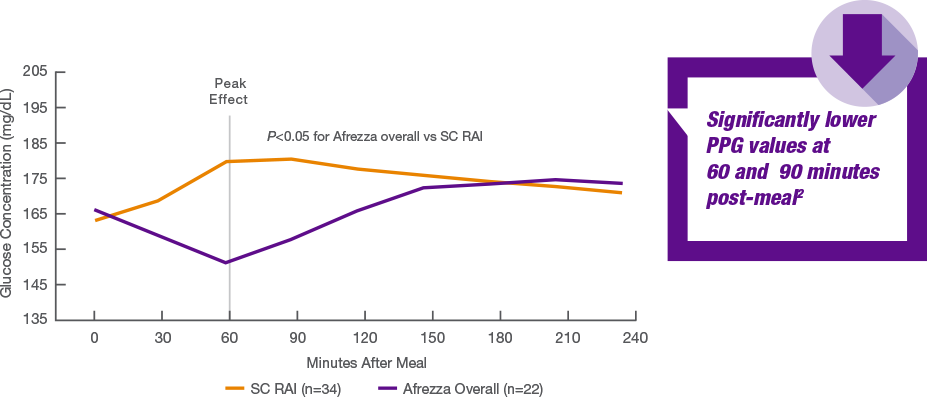 Why does anyone think this is going to different for an AID pump over Tresiba? The AID pump provides basal via RAA, and because the pump knows you have bolused it know there is insulin onboard to cover the food so it's not going to change the basal RAA and you get a flat basal curve, just like you would with Tresiba. This is a definitely not going to move the endos. The large scale ABC trial will be interesting, especially the Afrezza with food and pump the rest of the time arm. Here is the original STAT study chart. mnkd.proboards.com/thread/10239/dr-kendall-presents-stat-study1Scroll down |
|
|
|
Post by agedhippie on Feb 25, 2023 16:33:24 GMT -5
I realized I didn't answer the first part of that post! The graph curves are the same except that they are cut off after 2 hours unlike the STAT graph which ran for five hours. This was using a standardized meal under lab conditions, STAT was real world so the meal were wherever and anything but standardized You attach way to much importance to Nudge BG performing a consultancy engagement with Mannkind. If you hire an industry expert consultant that doesn't mean they are working with you beyond that engagement (or I am working for a ton of companies!) The stat showed how fearful type ones were to take a follow dose. You know afrezza needs the one hour follow up dose. There is an assumption there that it was fear rather than not being bothered. In my experience apathy is a more likely reason given that Type 1s routinely do correction doses with RAA. This comes back to my comment about not wanting something where I had to routinely do follow up doses because it got in the way of my life - I know I am not going to do it. This is also why I am interested in the ABC arm that uses insulin once with the meal and then lets the AID system clean up the leftovers. |
|
|
|
Post by agedhippie on Feb 25, 2023 16:34:47 GMT -5
MannKind to Give Oral Presentation on Meal Challenge Results From the Afrezza® With Basal Combination (ABC Study) at 16th Annual ATTD Conference today 2/25/23. Has any listened to this? I can't locate I don't think anything other than the abstract is available yet. Or rather I haven't been able to find a recording or transcript either! |
|
|
|
Post by sayhey24 on Feb 25, 2023 18:38:22 GMT -5
Correct - Mike said they were holding the main data for ADA2023. This is only afrezza with AID and AID without afrezza. This does not include Tresiba. What we can say is the graphs they presented are nothing like the graph you referred to earlier in the thread from STAT. I guess I can also say it makes sense Lance is now working with MNKD. There is no way he can write an alogorithm to beat this. ... I realized I didn't answer the first part of that post! The graph curves are the same except that they are cut off after 2 hours unlike the STAT graph which ran for five hours. This was using a standardized meal under lab conditions, STAT was real world so the meal were wherever and anything but standardized You attach way to much importance to Nudge BG performing a consultancy engagement with Mannkind. If you hire an industry expert consultant that doesn't mean they are working with you beyond that engagement (or I am working for a ton of companies!) Aged - here is the reality, there is no algorithm which Lance can write which will ever have the AID beat afrezza at 60minutes, 90minutes and I doubt 120 minutes. Al could not do it and Lane certainly is not. I do give Lance a lot of credit for deciding to work with MNKD. I think the MTTD work he is doing is very valuable. I am looking forward to the Tresiba numbers at ADA2023. If they are close to afrezza and AID, I would say we are looking at the new Standard of Care for T1s. The question is will Novo Nordisk get on board and promote this? If so afrezza has a fighting chance at changing the SoC. I know I would be kicking off the GLP1(Ozempic)/afrezza trial Mike mentioned ASAP and try and get NVO to partner. Mike needs to stop thinking about it and get something going. |
|
|
|
Post by peppy on Feb 25, 2023 19:37:49 GMT -5
Fast-acting insulin ( Humalog) starts working within 15 minutes after injection, peaks in about 1 to 2 hours after injection, and lasts between 2 to 4 hours after injection. www.humalog.com/fast-acting-mealtime-insulinInsulin aspart ( Novolog) has an onset of 10 to 20 minutes and a peak time of 40 to 50 minutes. The duration of insulin aspart is 3 to 5 hours. canadianinsulin.com/articles/insulin-aspart-onset-peak-time-duration-action-side-effects/Insulin lispro differs from human insulin by the substitution of proline with lysine in position 28 and lysine with proline in position 29 of the B chain; insulin aspart differs from human insulin by a single substitution of proline with aspartic acid in position B28. agedhippie, big difference in peak times? |
|
|
|
Post by peppy on Feb 25, 2023 20:12:30 GMT -5
Fast-acting insulin ( Humalog) starts working within 15 minutes after injection, peaks in about 1 to 2 hours after injection, and lasts between 2 to 4 hours after injection. www.humalog.com/fast-acting-mealtime-insulinInsulin aspart ( Novolog) has an onset of 10 to 20 minutes and a peak time of 40 to 50 minutes. The duration of insulin aspart is 3 to 5 hours. canadianinsulin.com/articles/insulin-aspart-onset-peak-time-duration-action-side-effects/Insulin lispro differs from human insulin by the substitution of proline with lysine in position 28 and lysine with proline in position 29 of the B chain; insulin aspart differs from human insulin by a single substitution of proline with aspartic acid in position B28. agedhippie , big difference in peak times? or Pharmacodynamics Studies in normal volunteers and patients with diabetes demonstrated that subcutaneous administration of NovoLog has a more rapid onset of action than regular human insulin. In a 6-hour study in patients with Type 1 diabetes (n=22), the maximum glucose-lowering effect of NovoLog occurred between 1 and 3 hours after subcutaneous injection (see Figure 3). The duration of action for NovoLog is 3 to 5 hours www.accessdata.fda.gov/drugsatfda_docs/label/2005/20986s032lbl.pdf |
|
|
|
Post by agedhippie on Feb 25, 2023 22:35:59 GMT -5
Feel free to correct me if I am not answering the question you are asking peppy. It reads like you are asking why these two RAA insulins have different PK/PD but are treated the same. I think the answer is because (and i have used both over the years) outside the lab they are effectively the same and their PK/PD vary from person to person. For me both have a noticeable tail out to six hours with 10% left at 5 hours. Endos believe the official PK/PD, diabetics know that it is highly individualized, but it should be in the ballpark. The variance is sufficiently small that you don't notice it and I say that as someone who fought tooth and nail when Aetna went Humalog only. There is an RAA from Sanofi called Apidra out there which apparently (I have never used it although I would like to have) is noticeably faster even if only marginally so according to people I trust. It was a popular pump insulin for those that could get insurance coverage which is very restricted. |
|
|
|
Post by agedhippie on Feb 25, 2023 22:50:26 GMT -5
Aged - here is the reality, there is no algorithm which Lance can write which will ever have the AID beat afrezza at 60minutes, 90minutes and I doubt 120 minutes. Al could not do it and Lane certainly is not. I do give Lance a lot of credit for deciding to work with MNKD. I think the MTTD work he is doing is very valuable. ... True, but it's just a meal. In the context of this data Afrezza will always win because you have a standard meal with no carbs already onboard - it's a very clean and simple use case. The real world is messy - I might have been snacking, had a coffee, still had the remains of an old meal (or two) in my system, been stressed, and so on. That's why AID matters because it can clean up that for you so your TIR is into the mid 70%. If I am just on Afrezza this is a problem because I need to perform that monitoring and dosing that the algorithm is doing automatically by hand and that's a lot of work! Real world numbers are what matter - it's why for me (although not so much the ADA!) things like the real world 780G numbers are so impressive. |
|
|
|
Post by lennymnkd on Feb 26, 2023 9:11:33 GMT -5
Is that monitoring the swipe of a phone ?
|
|
|
|
Post by hellodolly on Feb 26, 2023 9:59:08 GMT -5
Aged - here is the reality, there is no algorithm which Lance can write which will ever have the AID beat afrezza at 60minutes, 90minutes and I doubt 120 minutes. Al could not do it and Lane certainly is not. I do give Lance a lot of credit for deciding to work with MNKD. I think the MTTD work he is doing is very valuable. ... True, but it's just a meal. In the context of this data Afrezza will always win because you have a standard meal with no carbs already onboard - it's a very clean and simple use case. The real world is messy - I might have been snacking, had a coffee, still had the remains of an old meal (or two) in my system, been stressed, and so on. That's why AID matters because it can clean up that for you so your TIR is into the mid 70%. If I am just on Afrezza this is a problem because I need to perform that monitoring and dosing that the algorithm is doing automatically by hand and that's a lot of work! Real world numbers are what matter - it's why for me (although not so much the ADA!) things like the real world 780G numbers are so impressive. Excuse my confusion here but I have to ask because you present a great example for the reason why AIDs matter in the real world and I'm not a PWD. I see where you're coming from when it comes to having an AID maintain those real world "messy" BG levels. Not only at "mealtime" but any time, the AID can recognize an excursion and dose accordingly, I presume after either the onset has begun or at the peak of the excursion? Hence my confusion and assumption: Does an AID dose only at the peak level to begin the correction or does it dose smaller incremental amounts as it catches the excursion gaining traction during that messy day? Also, is there a need to still use a CGM if you utilize an AID? I would think so just to make sure you track your progress but, I'm not familiar with all of the features of an AID. Does it dose and track your BG? Keeping track of the BG levels seems to be the central piece to managing the disease. Moving on...I would believe when managing the disease, during those "messy moments" you illustrated, why Afrezza should also be included in that management tool kit and here's why. The old adage, "One size fits all does" cannot apply to this disease, period. Anything a PWD has available to manage their disease, because everyone is at different stages of managing the disease, requires a period of indoctrination into their new life (for those serious about managing the disease). Even as an outsider looking in and reading everything you and others post, one thing is absolutely a fact...this disease takes a HUGE learning curve. That learning does not come overnight and may take years to dial in what works best on an individual basis. Figure the challenges with adopting to the ongoing changes in science or what we know about food, the mechanics of nutrition and diet, the disease, the medical devices, the various insulins, dealing with doctors prejudices and bias towards the scientific literature, insurance networks, ages, education levels and maturity of the PWD's, life experiences, approach to the management of the disease, etc. This is why it's not as simple as, "Wear this it will save your life" or "Inhale at mealtime"...there's just too many variables, options, lifestyles that require each set of circumstances to define what suits and fits the individual best, given what I've stated. agedhippie you have provided me with such an education here in the last ~6 or 7 years. It does not go unnoticed and I'm grateful. My reply is in no way an attempt to teach you a lick about the life of a PWD. I have to much respect for you. It's just me letting it out that I cannot subscribe to the notion that Afrezza can be defeated at every turn, without feeling the same way about other therapies. There are too many unique moving parts with managing diabetes...it's not a static disease and Afrezza still has it's place in that tool box, regardless. Why? As discussed, there are many tools in that kit to choose from to manage the disease, but Afrezza is still the only ultra-fast rapid acting mealtime "inhaled insulin" available right now that provides PWDs an option to manage their BG with superior TIR outcomes and we will hear more from Mike on that very soon. IMHO, experienced PWD will choose for themselves what works best for them and they will not be pigeon holed into one therapy or another by their physicians anymore. |
|
|
|
Post by agedhippie on Feb 26, 2023 10:20:26 GMT -5
Is that monitoring the swipe of a phone ? No, that's reading the result. Monitoring is making the decision to pick up the phone and check. |
|



 You attach way to much importance to Nudge BG performing a consultancy engagement with Mannkind. If you hire an industry expert consultant that doesn't mean they are working with you beyond that engagement (or I am working for a ton of companies!)
You attach way to much importance to Nudge BG performing a consultancy engagement with Mannkind. If you hire an industry expert consultant that doesn't mean they are working with you beyond that engagement (or I am working for a ton of companies!)

