|
|
Post by peppy on Aug 14, 2016 9:25:17 GMT -5
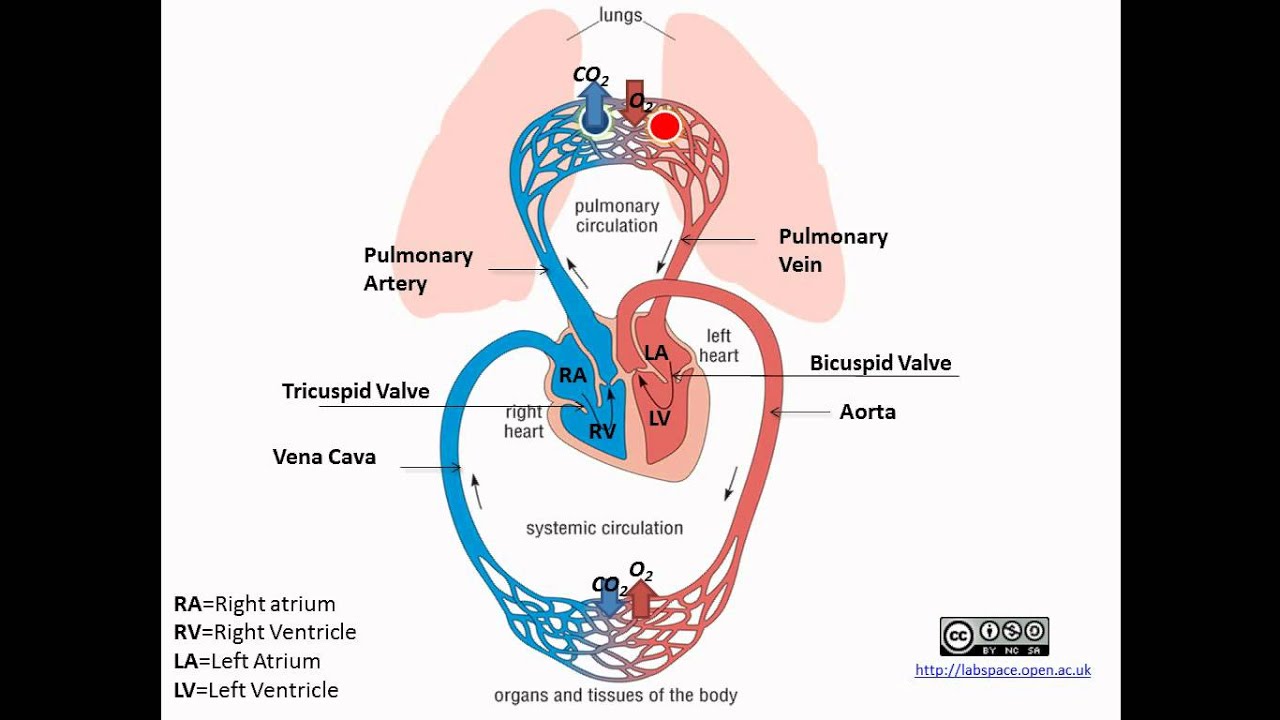
Really nobody who uses insulin cares if Afrezza gets it's speed through monomers, delivery route, or unicorns and magic. I'm pretty certain that the vast majority of insulin users have no idea how insulin forms. Once you start to talk about monomers you are talking about features and not benefits. Next thing you know you have to educate the market - this is a bad thing. The answer is it's fast, do you care why? That's a great comment, although as a bithead, I'm personally drawn to feeds & speeds like a moth to the flame. My opinion on all of this is that it's the mode of administration - inhalation - that makes the biggest difference since it gets the insulin into the blood stream right away. It's also what leads to the shorter tail vs SC insulin since the insulin is more immediately available to be utilized / broken down. With SC insulin, it is by design that the drug is made more gradually available (even for "fast acting" insulin) due to it having to seep out from fatty tissue into the blood stream. I suspect that intramuscular injection of rapid-acting insulin would show similar PK/PD to compared to Afrezza (see here: www.ncbi.nlm.nih.gov/pubmed/2140087 ), including quick in / quick out, but that's WAY off-label, and who knows what kind of hypo risk could ensue. I'm not about to test that theory... Alveoli The capillary bed flow. screencast.com/t/wWStocrld9
Pulmonary vein flows to the heart---> Liver...wham bang
|
|
ron
Newbie

Posts: 13 
|
Post by ron on Aug 14, 2016 9:43:14 GMT -5
I don't get why speed of onset is a selling point. The graph posted by "peppy" makes it look like a diabetic could just take lispro 15-20 minutes earier and get pretty much the same effect as afrezza.
|
|
|
|
Post by peppy on Aug 14, 2016 9:49:02 GMT -5
I don't get why speed of onset is a selling point. The graph posted by "peppy" makes it look like a diabetic could just take lispro 15-20 minutes earier and get pretty much the same effect as afrezza. look again. read the words


|
|
|
|
Post by agedhippie on Aug 14, 2016 9:56:21 GMT -5
Really nobody who uses insulin cares if Afrezza gets it's speed through monomers, delivery route, or unicorns and magic. I'm pretty certain that the vast majority of insulin users have no idea how insulin forms. Once you start to talk about monomers you are talking about features and not benefits. Next thing you know you have to educate the market - this is a bad thing. The answer is it's fast, do you care why? That's a great comment, although as a bithead, I'm personally drawn to feeds & speeds like a moth to the flame. My opinion on all of this is that it's the mode of administration - inhalation - that makes the biggest difference since it gets the insulin into the blood stream right away. It's also what leads to the shorter tail vs SC insulin since the insulin is more immediately available to be utilized / broken down. With SC insulin, it is by design that the drug is made more gradually available (even for "fast acting" insulin) due to it having to seep out from fatty tissue into the blood stream. I suspect that intramuscular injection of rapid-acting insulin would show similar PK/PD to compared to Afrezza (see here: www.ncbi.nlm.nih.gov/pubmed/2140087 ), including quick in / quick out, but that's WAY off-label, and who knows what kind of hypo risk could ensue. I'm not about to test that theory... I admit I am fascinated by the technicalities as well. The answer to your suspicions that intra-muscular injections would give a faster action is that you are correct. Biceps and quads are favorites if you are seriously high and want to drop fast. I have done it and contrary to the article I find it hurts although it is fast. I use it very very occasionally when no matter how much insulin I take things are not budging and I am getting desperate. Moving the limb around to activate the muscle helps as well, as does heat - anything to increase the blood flow to the muscle. Endos really do not like you doing IM injections, less because of the risks and more because they worry about needle breakages (a friend ended up with a needle in their thigh like that!) I am certain that it is the delivery rather than the insulin form that makes the difference. The evidence as I see it is that IV delivered Regular insulin, which is notorious for hexamers, exceeds onset and clearance for Afrezza. The peak from IV delivered Regular is almost instant because of rapid dispersal through the body the and the clearance half-life is around 10 minutes - compare that with SC delivered Regular! Afrezza is not as fast because it needs to reach the major body vessels from the outside in whereas IV delivered is directly. SC is slowest of all as it has to traverse interstitial fluid as well as the capillary blood vessels. |
|
|
|
Post by agedhippie on Aug 14, 2016 10:01:49 GMT -5
I don't get why speed of onset is a selling point. The graph posted by "peppy" makes it look like a diabetic could just take lispro 15-20 minutes earier and get pretty much the same effect as afrezza. You could, or you could take Regular even earlier. The thing is that it constrains when you can eat - I want that cupcake NOW and not in 20 minutes. (As a side note I find buttercream icing delays glucose spikes quite nicely for me.) You inject at the start of a meal because it minimizes the chance of your going low because the food is delayed. |
|
|
|
Post by peppy on Aug 14, 2016 10:17:35 GMT -5
That's a great comment, although as a bithead, I'm personally drawn to feeds & speeds like a moth to the flame. My opinion on all of this is that it's the mode of administration - inhalation - that makes the biggest difference since it gets the insulin into the blood stream right away. It's also what leads to the shorter tail vs SC insulin since the insulin is more immediately available to be utilized / broken down. With SC insulin, it is by design that the drug is made more gradually available (even for "fast acting" insulin) due to it having to seep out from fatty tissue into the blood stream. I suspect that intramuscular injection of rapid-acting insulin would show similar PK/PD to compared to Afrezza (see here: www.ncbi.nlm.nih.gov/pubmed/2140087 ), including quick in / quick out, but that's WAY off-label, and who knows what kind of hypo risk could ensue. I'm not about to test that theory... I admit I am fascinated by the technicalities as well. The answer to your suspicions that intra-muscular injections would give a faster action is that you are correct. Biceps and quads are favorites if you are seriously high and want to drop fast. I have done it and contrary to the article I find it hurts although it is fast. I use it very very occasionally when no matter how much insulin I take things are not budging and I am getting desperate. Moving the limb around to activate the muscle helps as well, as does heat - anything to increase the blood flow to the muscle. Endos really do not like you doing IM injections, less because of the risks and more because they worry about needle breakages (a friend ended up with a needle in their thigh like that!) I am certain that it is the delivery rather than the insulin form that makes the difference. The evidence as I see it is that IV delivered Regular insulin, which is notorious for hexamers, exceeds onset and clearance for Afrezza. The peak from IV delivered Regular is almost instant because of rapid dispersal through the body the and the clearance half-life is around 10 minutes - compare that with SC delivered Regular! Afrezza is not as fast because it needs to reach the major body vessels from the outside in whereas IV delivered is directly. SC is slowest of all as it has to traverse interstitial fluid as well as the capillary blood vessels. aged, probably getting phase 1 ... the insulin to the liver.... with IV insulin.. (?)
do you think this is in part some of the IV delivery effectiveness? one other thing. isn't it easy to in essence over dose IV? we would keep those pumps steady state, and be checking blood glucoses hourly.
|
|
|
|
Post by agedhippie on Aug 14, 2016 15:33:01 GMT -5
I admit I am fascinated by the technicalities as well. The answer to your suspicions that intra-muscular injections would give a faster action is that you are correct. Biceps and quads are favorites if you are seriously high and want to drop fast. I have done it and contrary to the article I find it hurts although it is fast. I use it very very occasionally when no matter how much insulin I take things are not budging and I am getting desperate. Moving the limb around to activate the muscle helps as well, as does heat - anything to increase the blood flow to the muscle. Endos really do not like you doing IM injections, less because of the risks and more because they worry about needle breakages (a friend ended up with a needle in their thigh like that!) I am certain that it is the delivery rather than the insulin form that makes the difference. The evidence as I see it is that IV delivered Regular insulin, which is notorious for hexamers, exceeds onset and clearance for Afrezza. The peak from IV delivered Regular is almost instant because of rapid dispersal through the body the and the clearance half-life is around 10 minutes - compare that with SC delivered Regular! Afrezza is not as fast because it needs to reach the major body vessels from the outside in whereas IV delivered is directly. SC is slowest of all as it has to traverse interstitial fluid as well as the capillary blood vessels. aged, probably getting phase 1 ... the insulin to the liver.... with IV insulin.. (?)
do you think this is in part some of the IV delivery effectiveness? one other thing. isn't it easy to in essence over dose IV? we would keep those pumps steady state, and be checking blood glucoses hourly.
The insulin will hit the liver very fast and that's what does it. My only experience of this is in DKA (only happened twice) where they used large bore access lines but mostly that was about the need to quickly push fluids (litres of the stuff!) and electrolytes to make up the losses. You are right about the pumps, the rate is set by weight and is constant, and the insulin starts acting really fast. The nurse was checking glucose every 15 minutes initially but then it changed to checking electrolytes and glucose hourly until everything was properly stable. They wouldn't let me sleep if I was below 140 and from memory they targeted around 180 using dextrose and insulin infusions. They overlay starting SC insulin with stopping IV insulin because if you stop one and start the other the IV insulin will clear before the SC insulin arrives. It was all rather exciting but I can't recommend it... DKA is far more dangerous than hypos but people don't usually talk about it. I have never been in the ER for a hypo but I have been in twice for DKA. The Type 2 version , HHS, is much rare but far more dangerous with a 15% mortality rate whereas DKA is around 0.2% if you get to hospital in time (if you don't it's fatal). |
|
|
|
Post by lakon on Aug 15, 2016 9:07:11 GMT -5
That's a great comment, although as a bithead, I'm personally drawn to feeds & speeds like a moth to the flame. My opinion on all of this is that it's the mode of administration - inhalation - that makes the biggest difference since it gets the insulin into the blood stream right away. It's also what leads to the shorter tail vs SC insulin since the insulin is more immediately available to be utilized / broken down. With SC insulin, it is by design that the drug is made more gradually available (even for "fast acting" insulin) due to it having to seep out from fatty tissue into the blood stream. I suspect that intramuscular injection of rapid-acting insulin would show similar PK/PD to compared to Afrezza (see here: www.ncbi.nlm.nih.gov/pubmed/2140087 ), including quick in / quick out, but that's WAY off-label, and who knows what kind of hypo risk could ensue. I'm not about to test that theory... I admit I am fascinated by the technicalities as well. The answer to your suspicions that intra-muscular injections would give a faster action is that you are correct. Biceps and quads are favorites if you are seriously high and want to drop fast. I have done it and contrary to the article I find it hurts although it is fast. I use it very very occasionally when no matter how much insulin I take things are not budging and I am getting desperate. Moving the limb around to activate the muscle helps as well, as does heat - anything to increase the blood flow to the muscle. Endos really do not like you doing IM injections, less because of the risks and more because they worry about needle breakages (a friend ended up with a needle in their thigh like that!) I am certain that it is the delivery rather than the insulin form that makes the difference. The evidence as I see it is that IV delivered Regular insulin, which is notorious for hexamers, exceeds onset and clearance for Afrezza. The peak from IV delivered Regular is almost instant because of rapid dispersal through the body the and the clearance half-life is around 10 minutes - compare that with SC delivered Regular! Afrezza is not as fast because it needs to reach the major body vessels from the outside in whereas IV delivered is directly. SC is slowest of all as it has to traverse interstitial fluid as well as the capillary blood vessels. Now, you are getting to the meat of the technology's delivery mechanism advancement. I dug into this point before. IV is the fastest, but who's going to do that on a regular basis? Sure it can be done, but it's got a lot of potential pitfalls and hazards, even under doctor supervision. IM is an option, but it has issues too. You should really use a bigger needle. Nobody wants that [Epi]. SC works, but it's inherently slower (capillary system). We all should know that Exubera does not perform as well as Afrezza so the form of insulin structure DOES MATTER. Put it together: inhaled + monomers AND the action is nearly identical to natural pancreatic response. Fast enough is fast enough. Afrezza/IV are fast enough, but SC is too slow. The fastest SC got there by using less stable forms of insulin (unnatural bio-synthetics). The next gen RAA will be even worse because they are solving the wrong problem -- burn thru the flesh faster. Use a more stable form of regular human insulin (monomers) [Afrezza], and take advantage of the technological advancement that IS Technosphere. derek2 there are different ways to parse Al Mann's statements, but you are wrong if you believe anybody, besides MNKD, stabilized human insulin monomers without forming hexamers. I recommend that you check the quality of your sources. What others did do was create new "unnatural" non-human insulin (analogs [RAA]) that are far less stable in hexameric form as regular human insulin hexamers. If you think that solves the problem for 400+ million and growing people with diabetes, think again. Long-term: cold chain logistics will be eliminated to service the entire population directly. That's how MNKD can accomplish Al Mann's final challenge. |
|
Deleted
Deleted Member
Posts: 0
|
Post by Deleted on Aug 15, 2016 9:12:16 GMT -5
all you folks get off my thread . you are polluting it :-)
|
|
|
|
Post by liane on Aug 15, 2016 9:15:33 GMT -5
@iam2sekc4u2002,
It would be better to politely ask people to return to the original intent of the thread.
|
|
Deleted
Deleted Member
Posts: 0
|
Post by Deleted on Aug 15, 2016 9:25:02 GMT -5
@iam2sekc4u2002, It would be better to politely ask people to return to the original intent of the thread. I didn't intend not to be polite.. Sorry if it came that way |
|
|
|
Post by peppy on Aug 15, 2016 9:33:22 GMT -5
|
|
Deleted
Deleted Member
Posts: 0
|
Post by Deleted on Aug 15, 2016 10:41:02 GMT -5
ok . All I wanted to know is , a pharmacy computer can check inventory levels at their distributor. WS puts a fancy term for this - Supply chain channel check. Can we not have that advantage?
|
|
Deleted
Deleted Member
Posts: 0
|
Post by Deleted on Aug 15, 2016 19:13:27 GMT -5
ok . All I wanted to know is , a pharmacy computer can check inventory levels at their distributor. WS puts a fancy term for this - Supply chain channel check. Can we not have that advantage? Any one? Isn't there some one? Why keep to yourself on the trends? |
|
|
|
Post by liane on Aug 15, 2016 19:27:14 GMT -5
Maybe there are no active pharmacists on this board. But if there are, they can always send you a PM if they prefer to remain undercover.
|
|






